可解释的多尺度深度学习在胸腔积液细胞块与细胞学涂片恶性肿瘤检测及侵袭性子宫内膜癌识别中的应用|文献速递-深度学习人工智能医疗图像
Title
题目
Interpretable multi-scale deep learning to detect malignancy in cell blocksand cytological smears of pleural effusion and identify aggressiveendometrial cancer
可解释的多尺度深度学习在胸腔积液细胞块与细胞学涂片恶性肿瘤检测及侵袭性子宫内膜癌识别中的应用
01
文献速递介绍
恶性胸膜积液的临床特征与深度学习诊断模型研究背景 恶性胸膜积液(MPE)的特征是积液中存在恶性细胞(Garcia-Pachon 等,2020)。MPE是转移性疾病患者的常见表现,约15%的癌症患者可能出现MPE(Bibby 等,2019;Feller-Kopman 等,2018)。当MPE发生时,通常表明癌症已进入晚期,预后较差,中位生存期仅约3至12个月(Desai 和 Lee,2017)。总体而言,观察性研究显示,出现MPE的患者,其死亡率显著高于未出现MPE的转移性癌症患者(Zamboni 等,2015)。因此,在临床实践中,快速且精准地诊断MPE对于评估预后和制定合理治疗方案至关重要。MPE细胞学检查在转移性癌症的诊断、治疗方案制定和病情监测中发挥着关键作用。当前国际指南推荐通过胸腔穿刺获取胸膜液进行细胞学检查,作为诊断MPE的方法(Hooper 等,2010)。然而,当胸膜液细胞学检查灵敏度较低时,阴性结果可能需要进一步采取有创检查,这会延误诊断与治疗进程。 穿刺抽吸是一种简便的诊断技术,细胞学涂片分析所提供的信息可帮助临床医生判断积液的可能病因,并辅助进行精准的鉴别诊断。细胞学检查有助于识别恶性细胞,但传统细胞学涂片可能面临诊断挑战:采用常规涂片方法时,难以区分细胞的良性与恶性改变,且诊断检出率相对较低(Santwani 等,2014)。在临床实践中,细胞块由剩余胸膜积液制备而成——通过离心或自然沉淀收集容器底部的凝块,用于后续分析。细胞块技术不仅操作简便,且侵袭性较低、可重复性好,对MPE的检出率也较高,因此在MPE的诊断和治疗指导中具有重要作用(Cheng 等,2015)。 几乎所有(95%)的MPE都由转移至胸膜腔的恶性肿瘤引起。约三分之二(70%–77%)的病例在组织学上归类为腺癌,其中以肺腺癌最为常见,其次是乳腺癌、淋巴瘤、妇科癌症和恶性间皮瘤(Lepus 和 Vivero,2018;Penz 等,2017)。对于这类患者,胸膜细胞学检查常作为临床判断肿瘤分期的首选诊断方法,且有可能获取肿瘤细胞用于进一步诊断或分子检测(Baburaj 等,2020;Akamatsu 等,2014;Ruan 等,2020)。在日常临床实践中,尽管许多晚期肺癌患者可通过胸膜积液细胞学检查确诊,但在胸膜积液细胞学诊断中,如何准确区分癌细胞与反应性间皮细胞仍是一大难题(Tosun 等,2015)。另一方面,采用免疫组化(IHC)染色可提高诊断准确性,但该方法并非适用于所有细胞学标本;若初始检查未检出恶性细胞,仍可能导致误诊。因此,细胞学涂片可能成为仅有的诊断样本,在这类情况下,细胞形态学特征就显得尤为重要。然而,对细胞形态学的主观观察可能导致观察者间一致性较低,即便对于经验丰富的病理医生,在复杂病例中也存在这一问题(Sakr 等,2012)。因此,提升区分MPE与良性胸膜积液(BPE)的能力具有重要意义。 本研究开发了一种基于自监督学习特征编码器的可解释多尺度注意力深度学习模型(IMA-SSL),用于分析胸膜积液细胞学涂片和细胞块全切片图像(WSI),旨在实现BPE与MPE病例的分类。为评估该模型的诊断性能,我们以患者病理报告作为诊断金标准,将所提方法与五种在计算病理学领域经证实有效的主流(SOTA)深度学习方法进行对比,包括经典多实例学习(MIL)(Campanella 等,2019)、聚类约束注意力多实例学习(CLAM)(Lu 等,2021b)、基于深度学习的肿瘤起源评估模型(TOAD)(Lu 等,2021a)、多尺度表征注意力网络(MRAN)(Xiang 等,2023)以及基于Transformer的多实例学习(TransMIL)(Shao 等,2021a)。
Abatract
摘要
The pleura is a serous membrane that surrounds the surface of the lungs. The visceral surface secretesfluid into the serous cavity, while the parietal surface ensures that the fluid is properly absorbed. However,when this balance is disrupted, it leads to the formation of pleural Effusion. The most common malignantpleural effusion (MPE) caused by lung cancer or breast cancer, and benign pleural effusions (BPE) causedby Mycobacterium tuberculosis infection, heart failure, or infections related to pneumonia. Today, with therapid advancement of treatment protocols, accurately diagnosing MPE has become increasingly important.Although cytology smears and cell blocks examinations of pleural effusion are the clinical gold standards fordiagnosing MPE, the diagnostic accuracy of these tools can be affected by certain limitations, such as lowsensitivity, diagnostic variability across different regions and significant inter-observer variability, leading to acertain proportion of misdiagnoses. This study presents a deep learning (DL) framework, namely InterpretableMulti-scale Attention DL with Self-Supervised Learning Feature Encoder (IMA-SSL), to identifyMPE or BPEusing 194 Cytological smears whole-slide images (WSIs) and 188 cell blocks WSIs. The use of DL on WSIs ofpleural effusion allows for preliminary results to be obtained in a short time, giving patients the opportunity forearlier diagnosis and treatment. The experimental results show that the proposed IMA-SSL consistently obtainedsuperior performance and outperformed five state-of-the-art (SOTA) methods in malignancy prediction on bothcell block and cytological smear datasets and also in identification of aggressive endometrial cancer (EC) usinga public TCGA dataset. Fisher’s exact test confirmed a highly significant correlation between the outputs ofthe proposed model and the slide status in the EC and pleural effusion datasets (𝐩 < 𝟎*.*𝟎𝟎𝟏), substantiating themodel’s predictive reliability. The proposed method has the potential for practical clinical application in theforeseeable future. It can directly detect the presence of malignant tumor cells from cost-effective cell blocksand pleural effusion cytology smears and facilitate personalized cancer treatment decisions
胸膜积液相关恶性肿瘤及侵袭性子宫内膜癌的深度学习诊断研究 胸膜是覆盖在肺表面的浆膜,脏层胸膜会向浆膜腔内分泌液体,而壁层胸膜则负责确保液体被正常吸收。然而,当这种分泌与吸收的平衡被打破时,就会引发胸膜积液。其中,最常见的恶性胸膜积液(MPE)多由肺癌或乳腺癌引起,良性胸膜积液(BPE)则常源于结核分枝杆菌感染、心力衰竭或肺炎相关感染。如今,随着治疗方案的快速发展,精准诊断恶性胸膜积液的重要性日益凸显。 尽管胸膜积液的细胞学涂片与细胞块检查是临床诊断恶性胸膜积液的“金标准”,但这些诊断手段存在一定局限性,例如灵敏度较低、不同地区诊断标准存在差异、观察者间诊断一致性差等,导致一定比例的误诊情况发生。本研究提出一种深度学习框架——基于自监督学习特征编码器的可解释多尺度注意力深度学习框架(IMA-SSL),并利用194张胸膜积液细胞学涂片全切片图像(WSI)和188张细胞块全切片图像(WSI),实现对恶性胸膜积液与良性胸膜积液的鉴别。将深度学习技术应用于胸膜积液全切片图像,可在短时间内获得初步诊断结果,为患者争取更早诊断和治疗的机会。 实验结果表明,所提出的IMA-SSL框架在细胞块数据集和细胞学涂片数据集的恶性肿瘤预测任务中,均展现出优于五种主流(SOTA)方法的性能;同时,在利用公共TCGA数据集进行侵袭性子宫内膜癌(EC)识别任务中,该框架同样表现突出。Fisher精确检验证实,在子宫内膜癌数据集和胸膜积液数据集中,该模型的输出结果与切片实际状态均存在高度显著相关性(p < 0.001),充分验证了模型的预测可靠性。 该方法在可预见的未来具有实际临床应用潜力,能够从成本效益较高的细胞块和胸膜积液细胞学涂片中直接检测恶性肿瘤细胞的存在,为癌症个性化治疗决策提供支持。
Method
方法
We introduced a weakly supervised Interpretable Multi-scale Attention DL with Self-Supervised Learning Feature Encoder (IMA-SSL),devised with multi-scale and multi-stage attention mechanisms to integrate and correlate multi-scale features in a WSI, to produce robustslide predictions without region-scale or manual pixel annotations (seeFig. 1). Firstly, the proposed method is structured across four hierarchical data representation scales (slide, bag, patch, and cell), therebyfacilitating the implementation of the proposed multi-scale attentionmechanism (see Section 3.1 and Fig. 1(a–c)). Secondly, for featureextraction, a Self-Supervised Residual Network (SSRNet) was developed to capture domain-specific features with a ResNet50 model. Formalignancy in cytological smears, the model was pre-trained on a largepathological unlabeled dataset using a SwAV SSL method to learnuseful representations, and for malignancy in cell blocks, pre-trained ona large pathological unlabeled dataset using a Barlow Twins (BT) SSLmethod to extract features (see Section 3.2 and Fig. 1(d)). Moreover,an efficient data augmentation strategy is described in Section 3.3.Thirdly, we presented an Interpretable Multi-scale Attention Module (IMAM) to harmoniously fetch crucial multi-scale information byintegrating and correlating Multi-scale features in a WSI while incorporating class distribution weight to deal with the imbalanced data(see Section 3.4), which outperforms all the latest SOTA DL MIL methods (Lu et al., 2021a; Xiang et al., 2023; Campanella et al., 2019;Lu et al., 2021b; Shao et al., 2021b) in this study (see Fig. 1(e)).Fourthly, a multi-stage Loss Function Model (MSLFM) is built to address class imbalance by incorporating multi-scale attention weightsto render individual stage loss values, including the bag loss at stageone and the slide loss (see Section 3.5 and Fig. 1(f)). MSLFM ensuresa balanced treatment of minority and majority classes as it helps tocompensate for the lack of data by giving more importance to theminority samples during training. Fifthly, we developed a Smart EarlyStopping Model Selector (SESM) for obtaining an optimal and efficientmodel while avoiding overfitting (see Section 3.6 and Fig. 1(g)). Lastly,we built a Multi-Scale Prediction Model (MSPM) to produce an accuratefinal slide-scale decision by integrating multi-scale attention weights(i.e. cell-, patch- and bag-scale weights) and individual bag decisionoutput (see Section 3.7 and Fig. 1(h)).
基于弱监督的可解释多尺度注意力深度学习模型(IMA-SSL)架构设计 本研究提出一种基于弱监督的、带有自监督学习特征编码器的可解释多尺度注意力深度学习模型(IMA-SSL)。该模型通过多尺度与多阶段注意力机制,整合并关联全切片图像(WSI)中的多尺度特征,无需区域级或人工像素级标注即可生成稳健的切片级预测结果(见图1)。其核心设计包含以下六个关键模块: ### 1. 四级分层数据表征架构 模型构建了“切片(slide)-包(bag)-补丁(patch)-细胞(cell)”四级分层数据表征尺度(详见3.1节及图1(a–c)),为后续多尺度注意力机制的实现提供结构基础——从整体切片到单个细胞,逐层细化特征捕捉维度,确保不同尺度下的病理信息均能被有效利用。 ### 2. 自监督残差网络(SSRNet)特征提取 为获取领域特异性特征,模型设计了自监督残差网络(SSRNet),并以ResNet50为基础网络: - 针对细胞学涂片恶性肿瘤检测:采用SwAV自监督学习(SSL)方法,在大规模未标注病理数据集上对模型进行预训练,以学习有效的特征表征; - 针对细胞块恶性肿瘤检测:采用Barlow Twins(BT)自监督学习方法,在另一大规模未标注病理数据集上完成预训练,实现特征提取(详见3.2节及图1(d))。 此外,3.3节还阐述了一种高效的数据增强策略,用于提升模型泛化能力。 ### 3. 可解释多尺度注意力模块(IMAM) 该模块通过整合并关联WSI中的多尺度特征,协同提取关键多尺度信息,同时引入类别分布权重以应对数据不平衡问题(详见3.4节及图1(e))。实验表明,该模块在本研究中性能优于所有最新主流深度学习多实例学习(MIL)方法(Lu等,2021a;Xiang等,2023;Campanella等,2019;Lu等,2021b;Shao等,2021b)。 ### 4. 多阶段损失函数模型(MSLFM) 为解决类别不平衡问题,模型构建了多阶段损失函数模型(MSLFM):通过融入多尺度注意力权重,生成各阶段的损失值,包括第一阶段的“包损失(bag loss)”与“切片损失(slide loss)”(详见3.5节及图1(f))。该模型在训练过程中对少数类样本赋予更高权重,补偿数据量不足的影响,确保少数类与多数类样本得到均衡处理。 ### 5. 智能早停模型选择器(SESM) 设计智能早停模型选择器(SESM),旨在筛选出最优且高效的模型,同时避免过拟合(详见3.6节及图1(g))——通过动态监测模型训练过程中的性能变化,在模型达到最佳泛化能力时及时停止训练,平衡模型性能与训练效率。 ### 6. 多尺度预测模型(MSPM) 构建多尺度预测模型(MSPM),通过整合多尺度注意力权重(即细胞级、补丁级、包级权重)与单个“包”的决策输出,生成精准的最终切片级诊断结果(详见3.7节及图1(h)),确保从局部特征到整体决策的有效关联,提升预测准确性。
Conclusion
结论
In our study, we developed an Interpretable Multi-scale AttentionDL with Self-Supervised Learning Feature Encoder (IMA-SSL) to detectmalignancy of pleural effusion using WSIs of cytology smear and cellblock slides. This method demonstrated high sensitivity in detectingmalignancy, which helps reduce the risk of false-negative cytologyresults in pleural effusion for clinicians. To date, although conventionalcancer biomarkers are widely used in the clinical assessment of pleuraleffusion, including carcinoembryonic antigen (CEA) (Nguyen et al.,2015; Shi et al., 2008) neuron-specific enolase (NSE) (Nguyen et al.,2015; Zhu et al., 2017), carbohydrate antigen 125 (CA125) (Nguyenet al., 2015; Liang et al., 2008), carbohydrate antigen 19-9 (CA19-
(Nguyen et al., 2015; Liang et al., 2008), and carbohydrate antigen15-3 (CA15-3) (Nguyen et al., 2015; Liang et al., 2008; Wu et al., 2015),the overall sensitivity of these traditional cancer biomarkers remainsunsatisfactory. Recently, several other nucleic acids in MPE have alsobeen identified—such as mesothelin, CYFRA 21-1, receptors on thesurface of immune cells (e.g., CD163+ on macrophages), extracellularmatrix proteins (e.g., OPN, Fibulin-3), RNA/DNA levels, and sequences.However, due to insufficient validation, the clinical application of thesebiomarkers is currently limited (Skok et al., 2019). Although cell-freemicroRNA in pleural effusion is considered to have potential as anovel diagnostic marker, the diagnostic accuracy of pleural effusionmicroRNA remains limited (Han et al., 2021).
本研究中IMA-SSL模型的研发背景与临床意义 在本研究中,我们开发了一种带有自监督学习特征编码器的可解释多尺度注意力深度学习模型(IMA-SSL),用于通过细胞学涂片和细胞块的全切片图像(WSI)检测胸膜积液的恶性肿瘤。该方法在恶性肿瘤检测中展现出较高的灵敏度,有助于为临床医生降低胸膜积液细胞学检查出现假阴性结果的风险。 迄今为止,尽管传统肿瘤生物标志物已被广泛用于胸膜积液的临床评估,包括癌胚抗原(CEA)(Nguyen等人,2015年;Shi等人,2008年)、神经元特异性烯醇化酶(NSE)(Nguyen等人,2015年;Zhu等人,2017年)、糖类抗原125(CA125)(Nguyen等人,2015年;Liang等人,2008年)、糖类抗原19-9(CA19-9)(Nguyen等人,2015年;Liang等人,2008年)以及糖类抗原15-3(CA15-3)(Nguyen等人,2015年;Liang等人,2008年;Wu等人,2015年),但这些传统肿瘤生物标志物的整体灵敏度仍不尽如人意。 近年来,研究人员还在恶性胸膜积液(MPE)中发现了其他多种核酸物质,例如间皮素、细胞角蛋白19片段(CYFRA 21-1)、免疫细胞表面受体(如巨噬细胞上的CD163+)、细胞外基质蛋白(如骨桥蛋白OPN、纤连蛋白-3 Fibulin-3)以及RNA/DNA的水平和序列等。然而,由于验证尚不充分,这些生物标志物目前的临床应用仍受到限制(Skok等人,2019年)。此外,尽管胸膜积液中的无细胞微小RNA(microRNA)被认为具有成为新型诊断标志物的潜力,但胸膜积液微小RNA的诊断准确性仍存在局限(Han等人,2021年)。
Results
结果
The proposed method was assessed using three independent datasetswith a total of 1300 de-identified WSIs, including a publicly availableEC dataset with 918 histopathology WSIs from TCGA for identificationof aggressive EC and two different kinds of pleural effusion datasetswith 194 cytological smear slides and 188 cell block slides, sourcedfrom the Tri-Service General Hospital (TSGH) Department of Pathologyfor malignancy detection (see Section 4.1 and Fig. 4). The experimentalresults show that the proposed IMA-SSL consistently achieved excellentperformance and outperformed five SOTA approaches in both identifying aggressive EC and detecting malignancy on cytological smears orcell block slides across three different datasets. (see Sections 4.2 and4.3). Moreover, statistical analysis using Fisher’s exact test confirmeda highly significant association between the proposed model predictionand the actual status in all three datasets (𝐩 < 𝟎*.*𝟎𝟎𝟏) (see Section 4.4).Furthermore, to examine the efficacy of individual components ofthe proposed IMA-SSL framework, extended ablation studies were performed, including comparisons of different (1) feature encoders usingthe EC Dataset (see Section 4.2.1 and Table 4(a)) and pleural effusiondatasets (see Section 4.3.1 and Table 6(a) and (b)), (2) model selectionmetrices using the EC Dataset (see Section 4.2.2 and Table 4(b)), (3)activation functions using the EC Dataset (see Section 4.2.3 and Table4(c)), (4) optimizer methods using the EC Dataset (see Section 4.2.4 andTable 4(d)) and pleural effusion datasets (see Section 4.3.2 and Table6(c) and (d)).
所提方法的数据集验证与消融实验设计 本研究采用三个独立数据集对所提方法进行评估,共包含1300张去标识化全切片图像(WSI),具体数据集信息及实验设计如下: ### 1. 实验数据集详情 - 侵袭性子宫内膜癌(EC)公开数据集:来源于TCGA数据库,包含918张组织病理学WSI,用于侵袭性子宫内膜癌的识别任务; - 胸膜积液数据集:来源于三军总医院(TSGH)病理科,包含两类样本——194张细胞学涂片切片与188张细胞块切片,均用于恶性肿瘤检测任务(详见4.1节及图4)。 ### 2. 核心实验结果 实验结果表明,所提出的IMA-SSL模型在三个不同数据集上均展现出优异性能:无论是在侵袭性子宫内膜癌识别任务中,还是在细胞学涂片/细胞块切片的恶性肿瘤检测任务中,其性能均优于五种主流(SOTA)方法(详见4.2节与4.3节)。此外,通过Fisher精确检验进行的统计分析证实,在所有三个数据集中,该模型的预测结果与样本实际状态均存在高度显著相关性(p < 0.001)(详见4.4节)。 ### 3. 扩展消融实验设计 为验证所提IMA-SSL框架各组成部分的有效性,本研究开展了扩展消融实验,具体对比维度如下: 1. 特征编码器对比:分别在子宫内膜癌数据集(详见4.2.1节及表4(a))与胸膜积液数据集(详见4.3.1节及表6(a)、(b))上,测试不同特征编码器对模型性能的影响; 2. 模型选择指标对比:在子宫内膜癌数据集上,验证不同模型选择指标的效果(详见4.2.2节及表4(b)); 3. 激活函数对比:在子宫内膜癌数据集上,分析不同激活函数对模型性能的作用(详见4.2.3节及表4(c)); 4. 优化器方法对比:分别在子宫内膜癌数据集(详见4.2.4节及表4(d))与胸膜积液数据集(详见4.3.2节及表6(c)、(d))上,比较不同优化器对模型训练效果的影响。
Figure
图
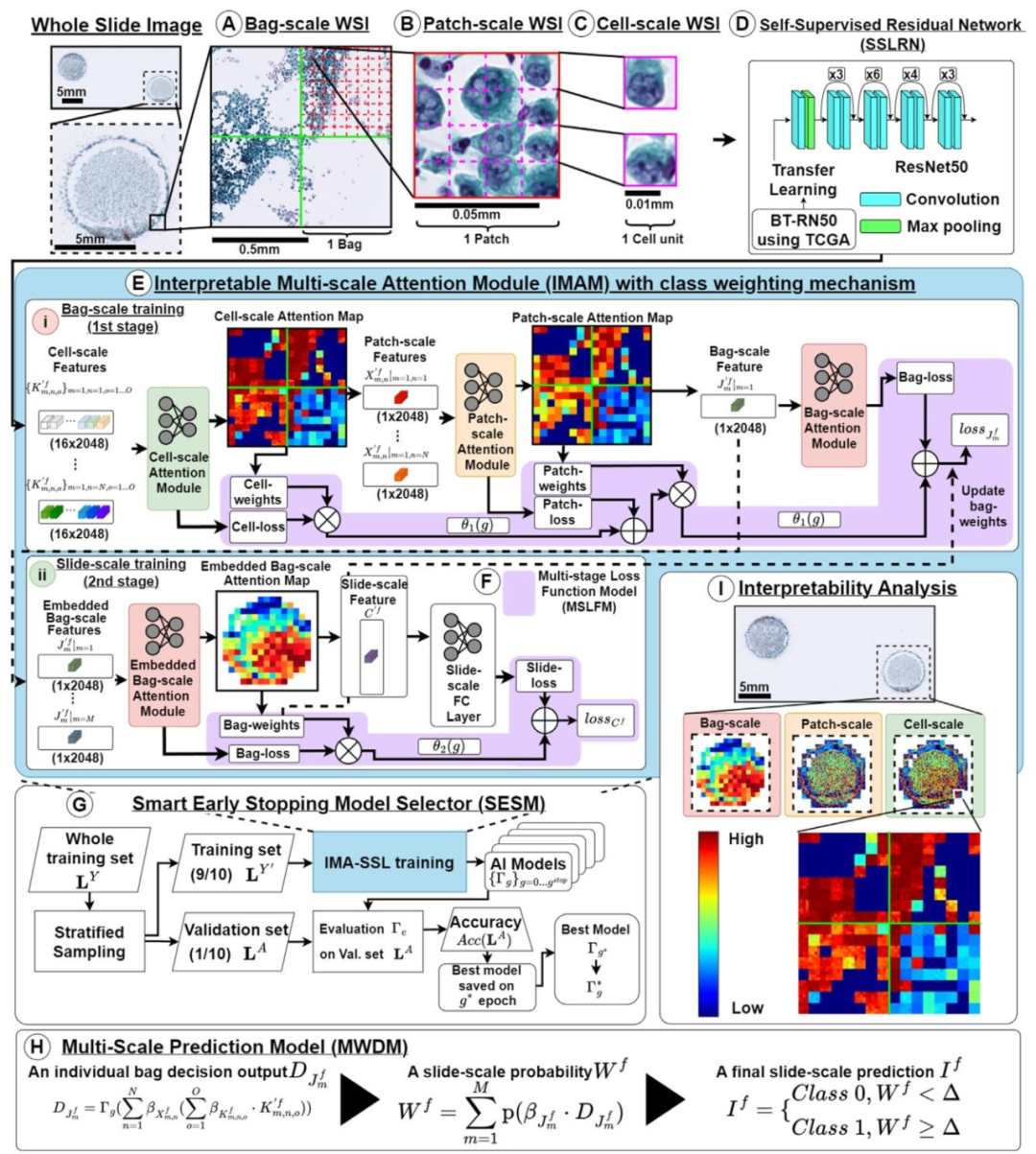
Fig. 1. Proposed Interpretable Multi-scale Attention DL with Self-Supervised Learning Feature Encoder (IMA-SSL): (A–C) Hierarchical Multi-scale Data Representation. (D) SelfSupervised Residual Network (SSRNet). (E) Interpretable Multi-scale Attention Module (IMAM) with class weighting mechanism. (F) Multi-stage Loss Function Model (MSLFM). (G)Smart Early Stopping Model Selector (SESM). (H) Multi-Scale Prediction Model (MSPM). (I) Model Interpretability Illustration.
图1 所提出的带有自监督学习特征编码器的可解释多尺度注意力深度学习模型(IMA-SSL): (A–C)分层多尺度数据表征;(D)自监督残差网络(SSRNet);(E)带有类别加权机制的可解释多尺度注意力模块(IMAM);(F)多阶段损失函数模型(MSLFM);(G)智能早停模型选择器(SESM);(H)多尺度预测模型(MSPM);(I)模型可解释性示意图
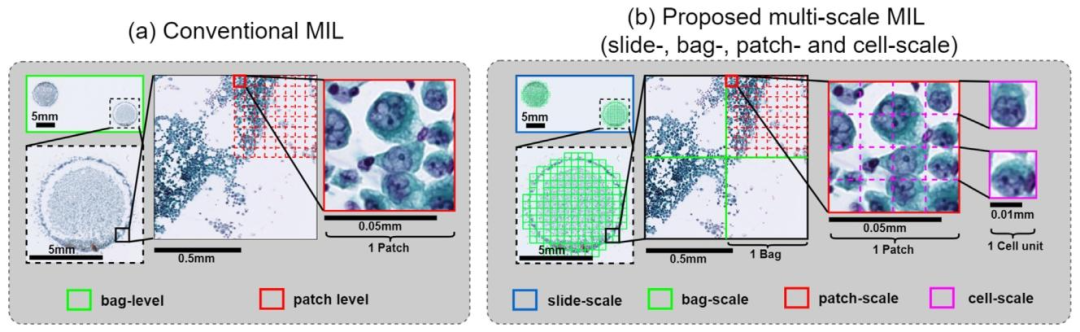
Fig. 2. Comparison of DL MIL method: (a) Conventional MIL method treats patches as instances and (b) Proposed Multi-scale MIL method treats cells as instances.
图2 深度学习多实例学习(DL MIL)方法对比:(a)传统多实例学习方法以补丁(patch)为实例;(b)所提多尺度多实例学习方法以细胞(cell)为实例
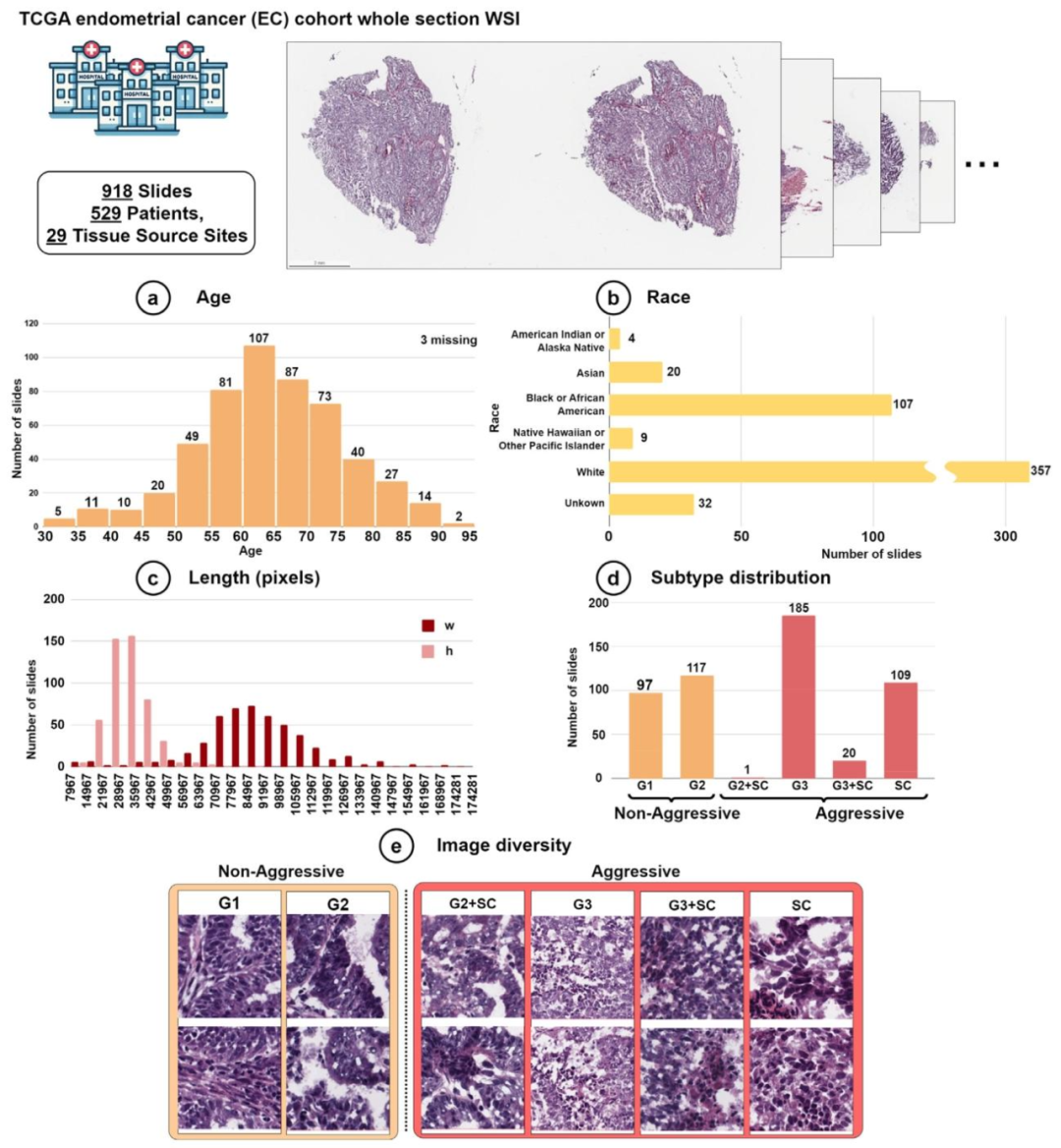
Fig. 3. Data information of the EC cohort. Data distribution in (a) Age, (b) Race, (c) Length (pixels), (d) Subtype distribution and (e) Image diversity.
图3 子宫内膜癌(EC)队列的数据集信息:(a)年龄分布、(b)种族分布、(c)图像长度(像素)分布、(d)亚型分布、(e)图像多样性
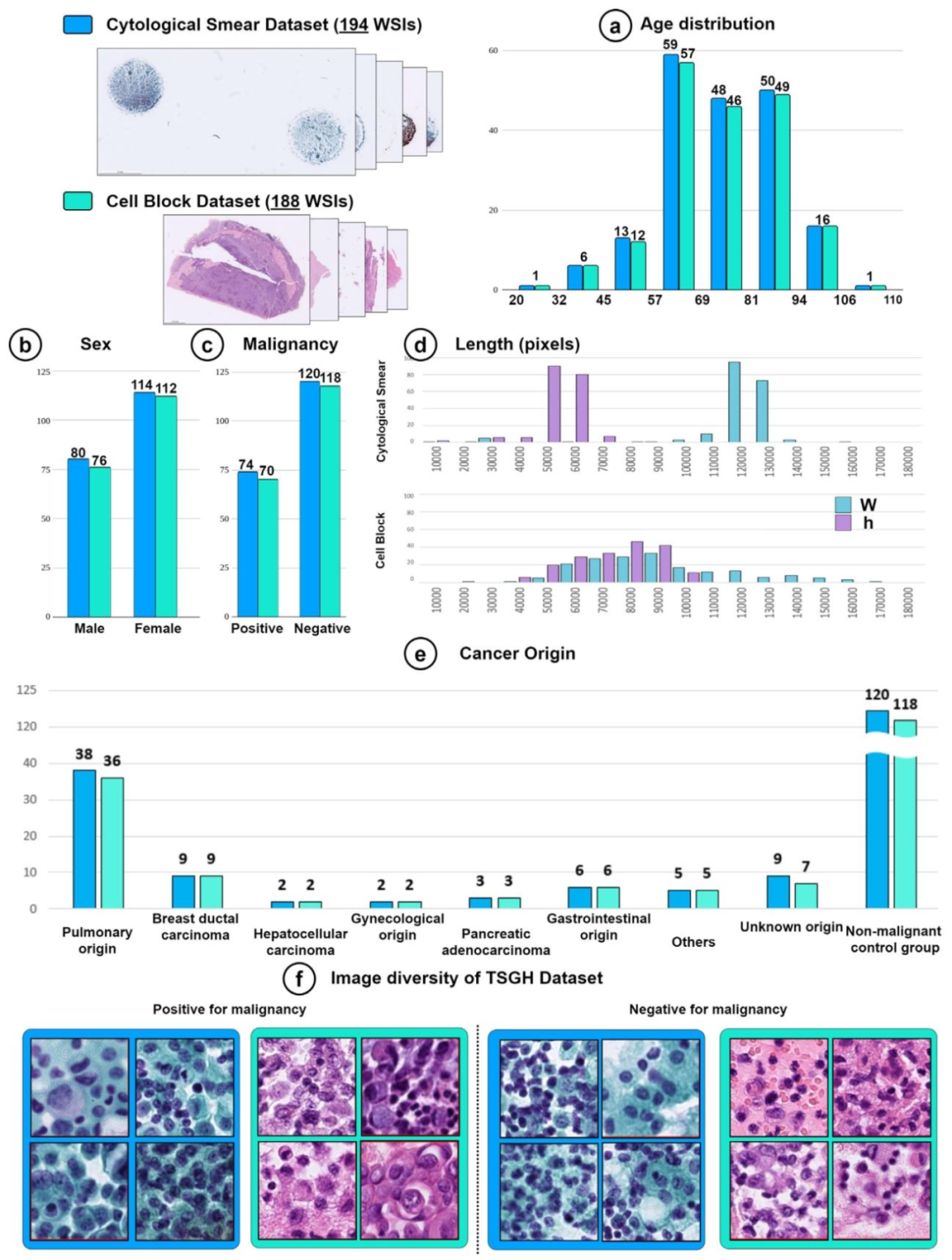
Fig. 4. Data information of the cytological smear and cell block datasets. Data distribution in (a) Age, (b) Sex, (c) Malignancy, (d) Length (pixels), (e) Cancer Origin and (f) Imagediversity
图4 细胞学涂片与细胞块数据集的信息:(a)年龄分布、(b)性别分布、(c)良恶性分布、(d)图像长度(像素)分布、(e)癌症起源分布、(f)图像多样性
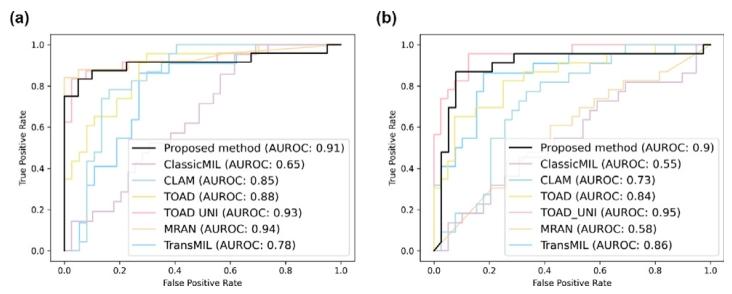
Fig. 5. Area Under the Receiver Operating Characteristic (AUROC) curves for malignancy prediction of pleural effusion using WSIs of (a) cytological smears and (b) cellblocks
图5 利用(a)细胞学涂片全切片图像(WSI)和(b)细胞块全切片图像(WSI)进行胸膜积液恶性肿瘤预测的受试者工作特征曲线下面积(AUROC)图
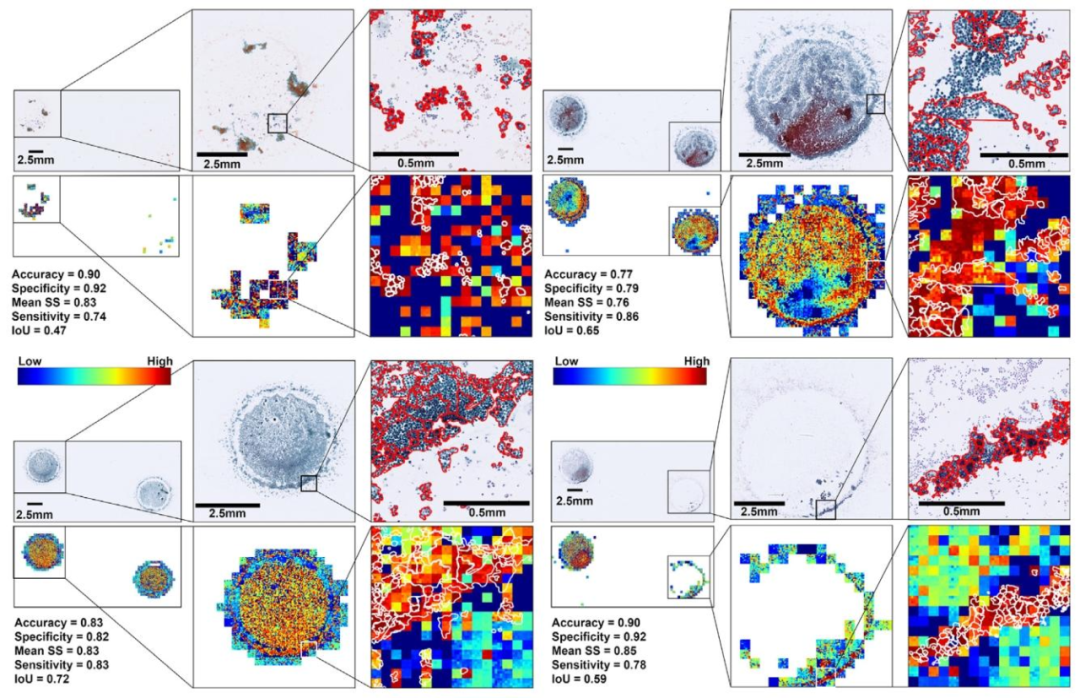
Fig. 6. Cell-scale attention heatmaps by the proposed method in malignancy prediction on cytological smears of pleural effusion.
图 6 所提方法在胸膜积液细胞学涂片恶性肿瘤预测中的细胞级注意力热力图
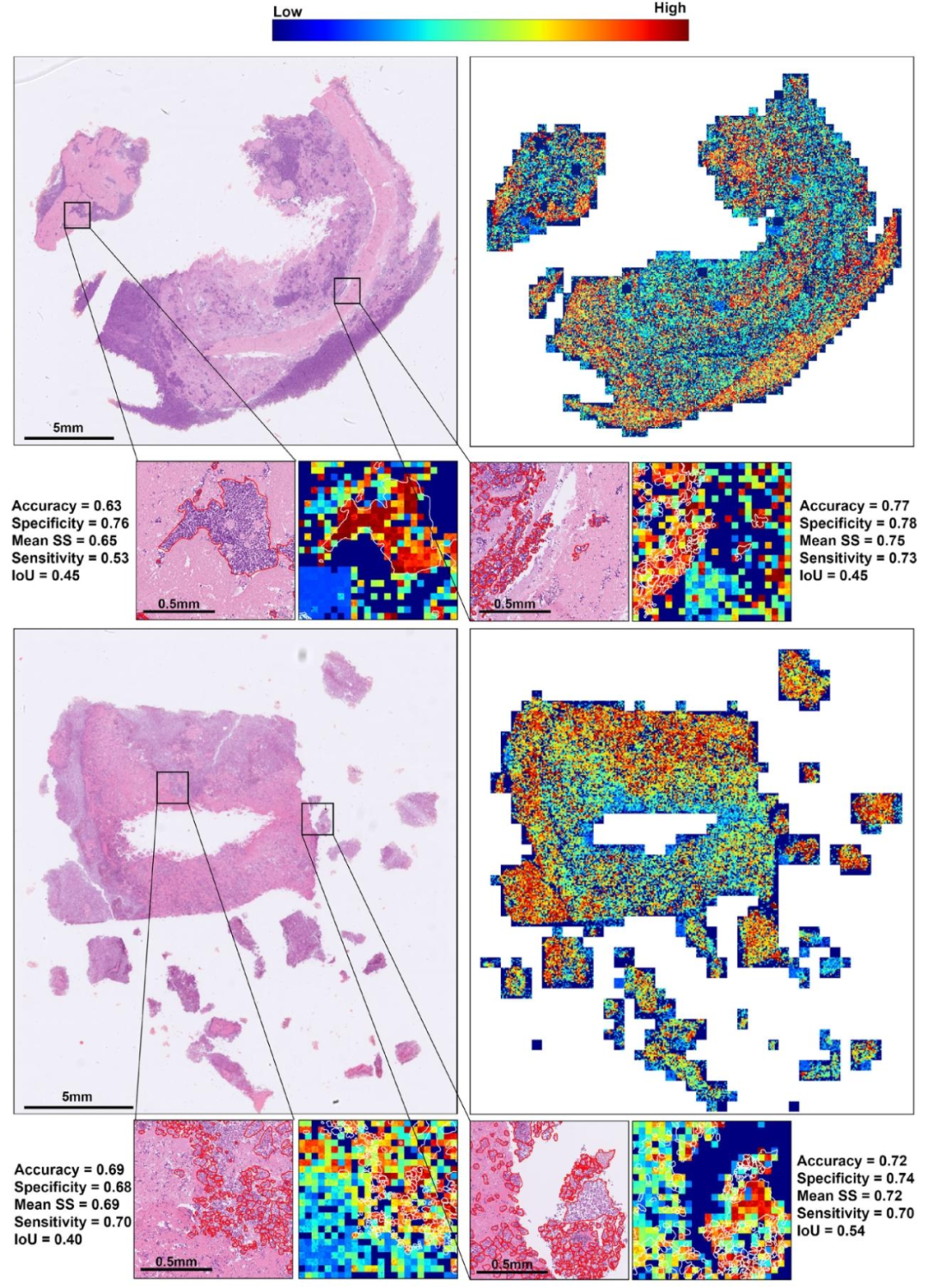
Fig. 7. Cell-scale attention heatmaps by the proposed method in malignancy prediction on cell blocks of pleural effusion.
图7 所提方法在胸膜积液细胞块恶性肿瘤预测中的细胞级注意力热力图
Table
表

Table 1Evaluation of data augmentation in the proposed framework
表 1 所提框架中数据增强的效果评估
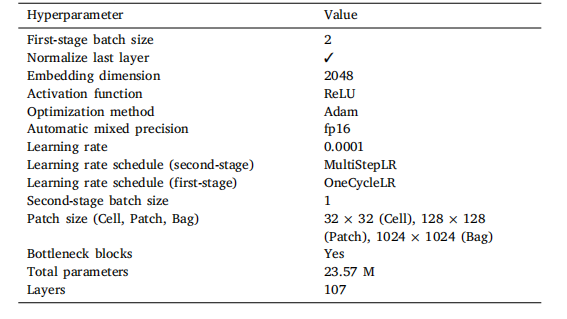
Table 2Details of the hyperparameter settings of the proposed IMA-SSL
表2 所提IMA-SSL模型的超参数设置详情
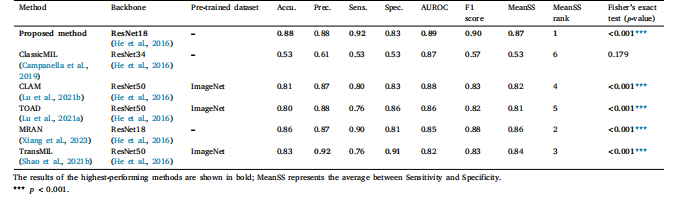
Table 3Evaluation of identification of aggressive and non-aggressive EC
表 3 侵袭性与非侵袭性子宫内膜癌(EC)的识别效果评估
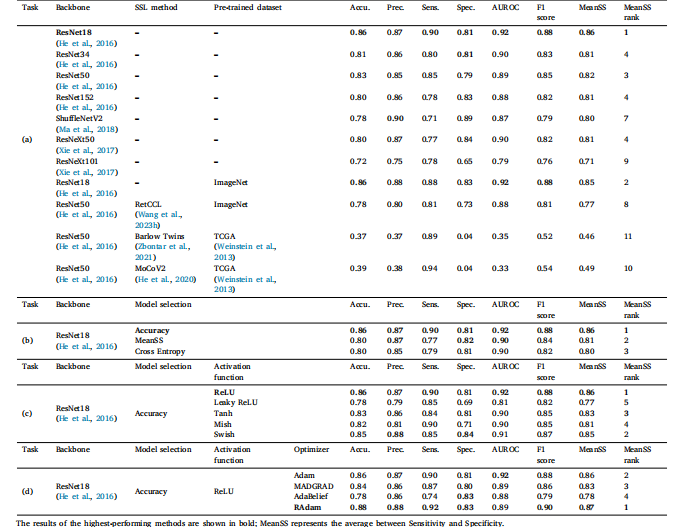
Table 4Comparison of (a) feature encoders, (b) model selection metrics, (c) activation functions, (d) optimizers in the proposed framework for identification of aggressive EC
表4 所提框架中用于侵袭性子宫内膜癌(EC)识别的(a)特征编码器、(b)模型选择指标、(c)激活函数、(d)优化器对比
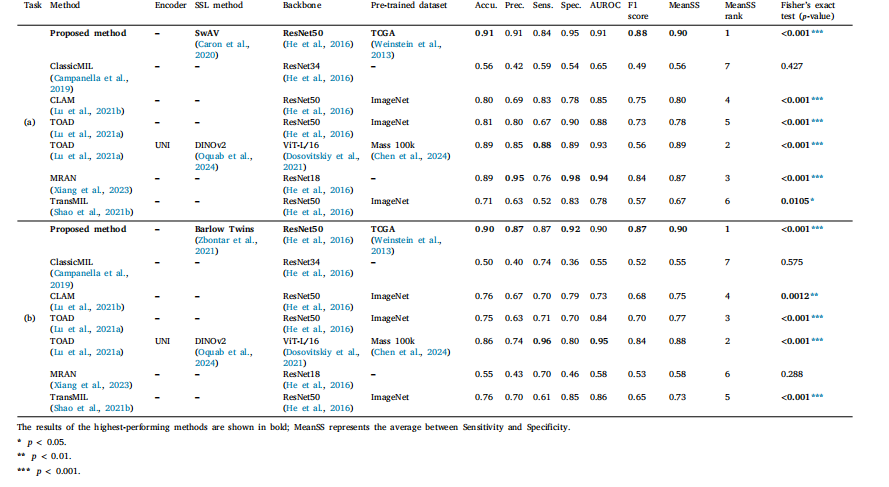
Table 5Evaluation of malignancy prediction in (a) cytological smears and (b) cell blocks of pleural effusion
表5 胸膜积液(a)细胞学涂片与(b)细胞块的恶性肿瘤预测效果评估
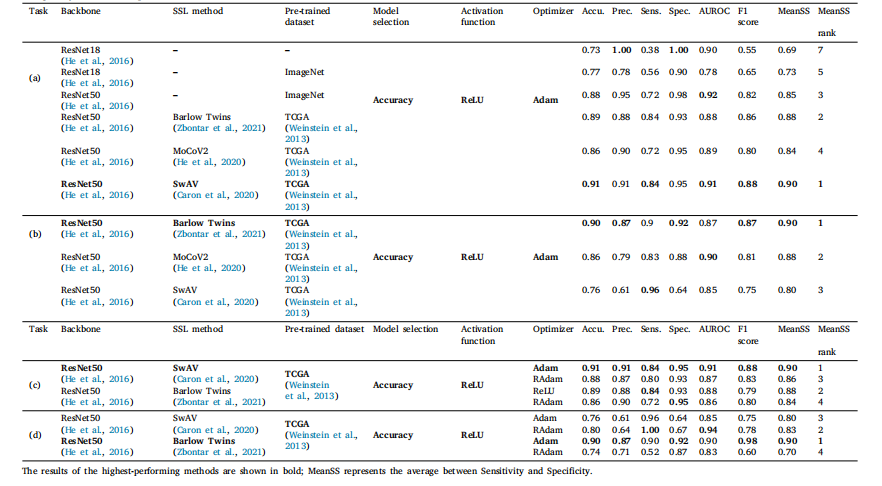
Table 6Comparison of feature encoders using (a) cytological smears and (b) cell blocks and optimizers using (c) cytological smears and (d) cell blocks in the proposed framework formalignancy detection of pleural effusion
表6 所提框架中用于胸膜积液恶性肿瘤检测的(a)细胞学涂片特征编码器对比、(b)细胞块特征编码器对比、(c)细胞学涂片优化器对比、(d)细胞块优化器对比
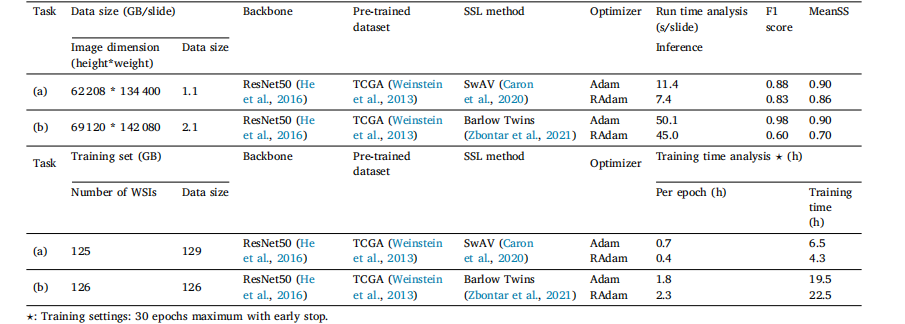
Table 7Runtime analysis of the proposed framework with different optimizers for malignancy detection in pleural effusion using (a) cytological smears and (b) cell blocks
表7 所提框架在使用不同优化器、基于(a)细胞学涂片和(b)细胞块进行胸膜积液恶性肿瘤检测时的运行时间分析