MBSS-T1:基于模型的特定受试者自监督运动校正方法用于鲁棒心脏 T1 mapping|文献速递-深度学习医疗AI最新文献
Title
题目
MBSS-T1: Model-based subject-specific self-supervised motion correction forrobust cardiac T1 mapping
MBSS-T1:基于模型的特定受试者自监督运动校正方法用于鲁棒心脏 T1 mapping
01
文献速递介绍
心脏T1定量成像(Quantitative Cardiac T1 Mapping)是一种先进的MRI技术,旨在精确测量心肌组织的固有纵向弛豫时间(Taylor等人,2016)。这一方法日益被视为评估弥漫性心肌疾病(如炎症、纤维化、肥厚和浸润)的关键手段(Taylor等人,2016;Van Zijl等人,1998)。无需顺磁性对比剂的“原生”心脏T1成像可有效检测心肌病变,包括水肿、铁过载、梗死和瘢痕(Schelbert和Messroghli,2016)。此外,通过对组织特征的客观量化,心脏T1成像能够对心肌变化进行纵向追踪,这对需要长期监测干预效果的临床试验具有重要价值(Schelbert和Messroghli,2016)。 图1展示了生成精确T1图的流程:首先在不同时间点采集一系列图像,每张图像捕捉纵向弛豫过程中的特定心肌状态,随后通过信号模型拟合计算T1弛豫时间,最终生成反映心肌组织特性的详细T1图。然而,心脏运动、呼吸及患者不自主移动可能导致T1图显著失真,影响其可靠性和临床实用性,甚至可能引发误诊(Tilborghs等人,2019)。基于心电图(ECG)信号的心脏触发是解决心脏运动影响的成熟方法,而屏气序列(如改良Look-Locker反转恢复序列MOLLI及其变体,Roujol等人,2014)常用于减少呼吸运动伪影。但要求患者屏气存在实际挑战——并非所有患者都能完全配合,且屏气采集限制了可获取的图像数量,使心脏T1成像不适用于无法耐受屏气的患者(Roujol等人,2014)。 通过图像配准对齐不同时间点的单次激发图像,可减少运动伪影并实现自由呼吸心脏T1成像。然而,由于图像数据存在固有复杂性(如对比度反转、部分容积效应,以及T1弛豫曲线过零点附近采集图像的信号归零现象,见图1),实现精确配准极具挑战性。 尽管基于经典算法和深度学习的运动校正及心脏T1成像方法已取得进展,但仍存在显著局限:传统基于模型的方法虽有效,但迭代特性导致计算效率低下(Tilborghs等人,2019;Xue等人,2012);深度学习方法则高度依赖大量标注数据集,而这类数据并非适用于所有扫描设备和协议(Gonzales等人,2021;Yang等人,2022)。此外,现有方法通常仅使用基于互信息等指标的成对损失函数引导配准过程(Arava等人,2021),或采用主成分分析(PCA)等组学方法,却忽略了信号衰减弛豫模型(Zhang等人,2024),这可能因图像对比度变化导致不符合物理规律的形变,进而影响方法的实用性和鲁棒性。 为此,本研究提出MBSS-T1,一种基于特定受试者的自监督、物理与解剖约束的深度学习模型,可同时实现屏气或自由呼吸采集中的运动校正与心脏T1成像。该方法融合物理与解剖学先验知识校正心脏T1成像中的运动误差,核心创新在于将信号模型直接嵌入特定受试者的自监督框架网络架构,并利用在STONE数据集(El-Rewaidy等人,2018;Fahmy,2019)上预训练的分割网络生成分割结果,引导配准过程以确保形变图像与参考帧的解剖学精确对齐。这一设计使模型能够跨多种成像协议生成抗运动干扰的心脏T1图,无需特定协议的数据采集、人工标注或大规模训练。本研究扩展了我们之前的监督学习模型PCMC-T1(Hanania等人,2023b)——后者依赖大量标注数据和深度训练,限制了其在不同采集场景(如序列类型、采集帧数)中的泛化能力。 我们通过五折实验验证了MBSS-T1在自由呼吸心脏T1成像中的优势,实验数据包括210例患者的公开自由呼吸定量数据集(采用STONE序列采集,El-Rewaidy等人,2018;Weingärtner等人,2015)和19例患者的内部数据集(采用MOLLI序列采集,涵盖自由呼吸和屏气扫描,Roujol等人,2014)。研究将MBSS-T1与基于深度学习的图像配准基线方法(Dalca等人,2019;Hoffmann等人,2021)及扫描仪生成的T1图进行对比,采用拟合质量(R²)、Dice系数和豪斯多夫距离作为定量指标评估配准精度和临床可用性,并通过放射科专家的定性评估验证其临床价值。
Abatract
摘要
Cardiac T1 mapping is a valuable quantitative MRI technique for diagnosing diffuse myocardial diseases.Traditional methods, relying on breath-hold sequences and cardiac triggering based on an ECG signal, facechallenges with patient compliance, limiting their effectiveness. Image registration can enable motion-robustcardiac T1 mapping, but inherent intensity differences between time points pose a challenge. We present MBSST1, a subject-specific self-supervised model for motion correction in cardiac T1 mapping. Physical constraints,implemented through a loss function comparing synthesized and motion-corrected images, enforce signal decaybehavior, while anatomical constraints, applied via a Dice loss, ensure realistic deformations. The uniquecombination of these constraints results in motion-robust cardiac T1 mapping along the longitudinal relaxationaxis. In a 5-fold experiment on a public dataset of 210 patients (STONE sequence) and an internal dataset of19 patients (MOLLI sequence), MBSS-T1 outperformed baseline deep-learning registration methods. It achievedsuperior model fitting quality (𝑅2 : 0.975 vs. 0.941, 0.946 for STONE; 0.987 vs. 0.982, 0.965 for MOLLI freebreathing; 0.994 vs. 0.993, 0.991 for MOLLI breath-hold), anatomical alignment (Dice: 0.89 vs. 0.84, 0.88 forSTONE; 0.963 vs. 0.919, 0.851 for MOLLI free-breathing; 0.954 vs. 0.924, 0.871 for MOLLI breath-hold), andvisual quality (4.33 vs. 3.38, 3.66 for STONE; 4.1 vs. 3.5, 3.28 for MOLLI free-breathing; 3.79 vs. 3.15, 2.84 forMOLLI breath-hold). MBSS-T1 enables motion-robust T1 mapping for broader patient populations, overcomingchallenges such as suboptimal compliance, and facilitates free-breathing cardiac T1 mapping without requiringlarg
心脏T1 mapping是一种用于诊断弥漫性心肌疾病的有价值的定量MRI技术。传统方法依赖屏气序列和基于心电图(ECG)信号的心脏触发,面临患者配合度的挑战,限制了其有效性。图像配准技术可实现对运动鲁棒的心脏T1 mapping,但时间点之间的固有强度差异构成了一项挑战。我们提出了MBSS-T1,一种用于心脏T1 mapping运动校正的特定受试者自监督模型。通过损失函数(比较合成图像与运动校正图像)实现的物理约束,强制信号衰减行为;通过Dice损失应用的解剖约束,确保真实的形变。这些约束的独特结合,实现了沿纵向弛豫轴对运动鲁棒的心脏T1 mapping。 在210例患者的公共数据集(STONE序列)和19例患者的内部数据集(MOLLI序列)上进行的五折实验中,MBSS-T1优于基线深度学习配准方法。其在模型拟合质量(R²:STONE序列为0.975 vs. 0.941、0.946;MOLLI自由呼吸序列为0.987 vs. 0.982、0.965;MOLLI屏气序列为0.994 vs. 0.993、0.991)、解剖对齐(Dice系数:STONE序列为0.89 vs. 0.84、0.88;MOLLI自由呼吸序列为0.963 vs. 0.919、0.851;MOLLI屏气序列为0.954 vs. 0.924、0.871)和视觉质量(STONE序列为4.33 vs. 3.38、3.66;MOLLI自由呼吸序列为4.1 vs. 3.5、3.28;MOLLI屏气序列为3.79 vs. 3.15、2.84)方面均表现更优。MBSS-T1为更广泛的患者群体实现了对运动鲁棒的T1 mapping,克服了配合度不佳等挑战,并无需大量数据即可促进自由呼吸心脏T1 mapping。
Method
方法
The T1 recovery time can be modeled using distinct equations tailored to the specific sequences employed for signal measurement. Theoverall signal recovery for inversion recovery and Look-Locker-basedmeasurements can generally be described as follows:𝐼(𝑡*) = 𝐴 − 𝐵 ⋅ 𝑒 −𝑡∕𝑇 1(1)where 𝐼(𝑡) is the magnitude image reconstructed from the multi-coilraw data obtained at time 𝑡.For the modified Look-Locker inversion recovery (MOLLI) sequence,𝐴 and 𝐵 are fitting parameters related to the equilibrium magnetizationand type of preparation, 𝑡 is the time after the preparation (i.e. inversion), and 𝑇 1 ∗ is the apparent 𝑇 1 which needs to be further correctedto get the actual tissue 𝑇 1 using the following equation (Taylor et al.,2016):𝑇 1 = 𝑇 1 ∗ ⋅ (𝐵∕𝐴 − 1) (2)
For the slice-interleaved T1 (STONE) sequence, the two-parameter signal recovery model (i.e. assuming a perfect efficiency of the inversionpulses) can be derived from Eq. (1) as follows: 𝐴 can be substitutedby the equilibrium magnetization 𝑀0 which is the magnetization ofthe tissue before any preparation occurs, 𝐵 by 2𝑀0 , and 𝑇 1 ∗ by theactual 𝑇 1 to get the proper signal recovery equation for this sequence(Weingärtner et al., 2015):𝐼(𝑡) = 𝑀0 ⋅ ( 1 − 2 ⋅ 𝑒 −𝑡∕𝑇 1 )(3)
T1恢复时间可通过针对信号测量所采用的特定序列定制的不同方程进行建模。对于反转恢复和基于Look-Locker的测量,总体信号恢复通常可描述如下: [ I(t) = A - B \cdot e^{-t/T_1} ] (1) 其中,( I(t) ) 是从时间 ( t ) 获得的多线圈原始数据重建的幅度图像。 对于改良型Look-Locker反转恢复(MOLLI)序列,( A ) 和 ( B ) 是与平衡磁化强度和预处理类型相关的拟合参数,( t ) 是预处理(即反转)后的时间,( T_1^* ) 是表观T1值,需要使用以下公式进一步校正以获得实际组织T1值(Taylor等人,2016): [ T_1 = T_1^* \cdot \left( \frac{B}{A} - 1 \right) ] (2) 对于层间交错T1(STONE)序列,双参数信号恢复模型(即假设反转脉冲效率完美)可由公式(1)推导如下:( A ) 可替换为平衡磁化强度 ( M_0 )(即预处理前的组织磁化强度),( B ) 替换为 ( 2M_0 ),( T_1^* ) 替换为实际 ( T_1 ),从而得到该序列的信号恢复方程(Weingärtner等人,2015): [ I(t) = M_0 \cdot \left( 1 - 2 \cdot e^{-t/T_1} \right) ] (3)
Conclusion
结论
In this study, we proposed MBSS-T1, a subject-specific, selfsupervised motion correction method for robust cardiac T1 mapping.By integrating physical constraints through a signal model and anatomical constraints via segmentation, MBSS-T1 effectively mitigates motion artifacts in both free-breathing and breath-hold acquisitions. Themethod demonstrated superior performance compared to baseline approaches, producing more homogeneous T1 maps and achieving higherclinical scores and segmentation metrics. Importantly, the selfsupervised nature of MBSS-T1 enables its adaptability to diverse imaging protocols without requiring large annotated datasets. Future workwill focus on addressing current limitations, including exploring advanced motion modeling and optimization strategies, to further enhance the method’s robustness and clinical applicability.
在本研究中,我们提出了MBSS-T1,一种针对特定受试者的自监督运动校正方法,用于实现鲁棒的心脏T1 mapping。通过信号模型整合物理约束并通过分割引入解剖约束,MBSS-T1可有效缓解自由呼吸和屏气采集中的运动伪影。与基线方法相比,该方法表现出更优的性能,生成的T1图更均匀,并获得了更高的临床评分和分割指标。重要的是,MBSS-T1的自监督特性使其能够适应多种成像协议,无需大量标注数据集。未来的工作将聚焦于解决当前局限性,包括探索先进的运动建模和优化策略,以进一步增强该方法的鲁棒性和临床适用性。
Results
结果
Fig. 3 presents the distribution of the selected reference time pointsacross different acquisition methods (BH-MOLLI, FB-MOLLI, and FBSTONE) by our MBSS-T1 approach. The majority of selections occurat time point 0 across all methods (BH-MOLLI, FB-MOLLI, and FBSTONE). These findings suggest that the reference state is predominantly chosen in the mid-diastolic phase.5.1. Exp. 1: Motion correction in free-breathing MRI using STONE datasetQuantitative evaluation: Table 1 summarizes our results for thetest sets across all folds, encompassing a total of 210 patients. TheMBSS-T1STONE method outperformed other state-of-the-art registrationmethods in terms of 𝑅2 , Dice score, and Hausdorff distance. Specifically, MBSS-T1STONE achieved an 𝑅2 value of 0.975 ± 0.05, whichrepresents an improvement of approximately 3% compared to thenext best method, PCMC-T1, with an 𝑅2 of 0.955 ± 0.078. Additionally, MBSS-T1STONE produced a Dice score of 0.89 ± 0.075, surpassing SynthMorph’s 0.88 ± 0.149, and reduced the Hausdorff distanceto 6.43 ± 5.54 mm, which is a 31% improvement compared to SynthMorph’s 8.59 ± 9.98 mm. These results suggest that our approachenhances the physical plausibility of deformations through signal relaxation and anatomical consistency. Our results are particularly noteworthy, considering we compared methods requiring a full trainingprocess.Fig. 4 depicts the deformed images alongside the predicted deformation fields for the different methods. Our MBSS-T1 approachgenerates smoother grids with visually realistic deformations, whereasSynthMorph produces less realistic deformation patterns.Table 2 summarizes the results of the Jacobian determinant analysis. Our MBSS-T1 approach produces deformation fields with a lowmean number of folds (0.0052 ± 0.111) and a mean Jacobian determinant close to 1 (0.9969 ± 0.0043), indicating more realistic deformation
Clinical impact: Fig. 5 presents several representative cases. Themaps generated by the MBSS-T1STONE method demonstrate the highestquality, as evidenced by superior metrics. The rightmost column ofTable 1 summarizes the clinical impact assessment results for the MBSST1STONE method, which achieved the highest quality score of 4.33±0.54.This score reflects an improvement of approximately 10% over thefollowing best method, PCMC-T1, which had a score of 3.93 ± 0.78.The difference in radiologist grading was statistically significant (p≪* 10−5). Furthermore, as demonstrated in Fig. 6, the MBSS-T1STONEmethod achieves a closer fit to the expected magnetization curve (with𝑅2 = 0.*99) and reduces artifacts, which may contribute to improved diagnostic confidence. These results suggest the MBSS-T1STONE method’spotential utility in clinical settings where motion artifacts can impactthe accuracy of cardiac T1 mapping.
图3展示了MBSS-T1方法在不同采集方式(屏气MOLLI、自由呼吸MOLLI和自由呼吸STONE)中所选参考时间点的分布。所有方法(BH-MOLLI、FB-MOLLI和FB-STONE)中,大多数选择发生在时间点0。这些发现表明,参考状态主要选择在舒张中期。 5.1 实验1:使用STONE数据集在自由呼吸MRI中进行运动校正 #### 定量评估 表1总结了所有折叠测试集的结果,共涵盖210名患者。MBSS-T1STONE方法在R²、Dice系数和豪斯多夫距离方面优于其他最先进的配准方法。具体而言,MBSS-T1STONE的R²值为0.975±0.05,比次优方法PCMC-T1(R²=0.955±0.078)提高了约3%。此外,MBSS-T1STONE的Dice系数为0.89±0.075,超过了SynthMorph的0.88±0.149,并将豪斯多夫距离减少到6.43±5.54 mm,比SynthMorph的8.59±9.98 mm改善了31%。这些结果表明,我们的方法通过信号弛豫和解剖一致性增强了变形的物理合理性。考虑到我们比较的是需要完整训练过程的方法,我们的结果尤其值得注意。 图4描绘了不同方法的变形图像和预测变形场。我们的MBSS-T1方法生成的网格更平滑,变形在视觉上更真实,而SynthMorph产生的变形模式则不太真实。 表2总结了雅可比行列式分析的结果。我们的MBSS-T1方法产生的变形场平均折叠次数较少(0.0052±0.111),平均雅可比行列式接近1(0.9969±0.0043),表明变形更真实。 临床影响* 图5展示了几个代表性病例。MBSS-T1STONE方法生成的图谱质量最高,指标优异。表1最右列总结了MBSS-T1STONE方法的临床影响评估结果,其质量评分最高,为4.33±0.54,比次优方法PCMC-T1(评分3.93±0.78)提高了约10%。放射科医生评分的差异具有统计学意义(p≪10⁻⁵)。此外,如图6所示,MBSS-T1STONE方法更接近预期的磁化曲线(R*²=0.99),并减少了伪影,这可能有助于提高诊断信心。这些结果表明,MBSS-T1STONE方法在运动伪影可能影响心脏T1 mapping准确性的临床环境中具有潜在实用性。
Figure
图
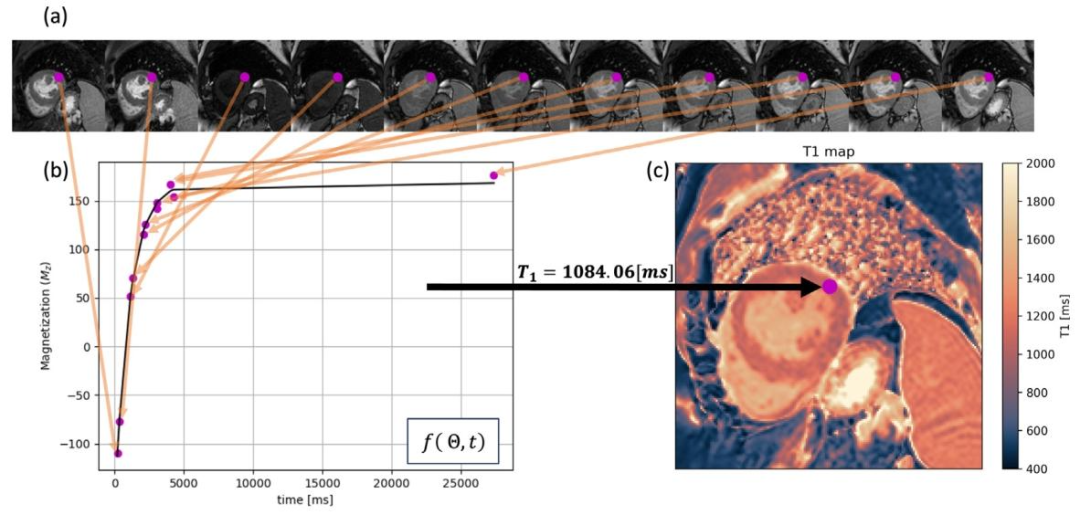
Fig. 1. Schematic representation of cardiac T1 mapping for a single voxel. (a) T1-weighted myocardial images acquired at 𝑁 − 1 sequential time points. (b) Fitting an inversionrecovery curve 𝑓 (𝛩, 𝑡) of the longitudinal magnetization across time points 𝑡 to estimate the corresponding parameters 𝛩. In this STONE sequence with the two-parameter model,𝛩= {𝑀0 , 𝑇 1} and 𝑓 (𝛩, 𝑡) = 𝑀0 ⋅ ( 1 − 2 ⋅ 𝑒 −𝑡∕𝑇 1 ) , where 𝑀0 represents the equilibrium magnetization, which is the tissue magnetization before any preparation, and 𝑇 1 reflects theactual T1 value. (c) Computed T1 map visualizing the estimated T1 values across the myocardium
图1. 单个体素心脏T1 mapping示意图 (a)在𝑁−1个连续时间点采集的T1加权心肌图像。 (b)通过拟合纵向磁化强度随时间点𝑡变化的反转恢复曲线𝑓(𝛩, 𝑡),估计相应参数𝛩。在基于双参数模型的STONE序列中,𝛩= {𝑀₀, 𝑇₁},且𝑓(𝛩, 𝑡) = 𝑀₀⋅(1−2⋅𝑒⁻ᵗ⁄ᵀ¹),其中𝑀₀表示平衡磁化强度(即任何预处理前的组织磁化强度),𝑇₁反映实际T1值。 (c)计算得到的T1图,可视化心肌各处估计的T1值。
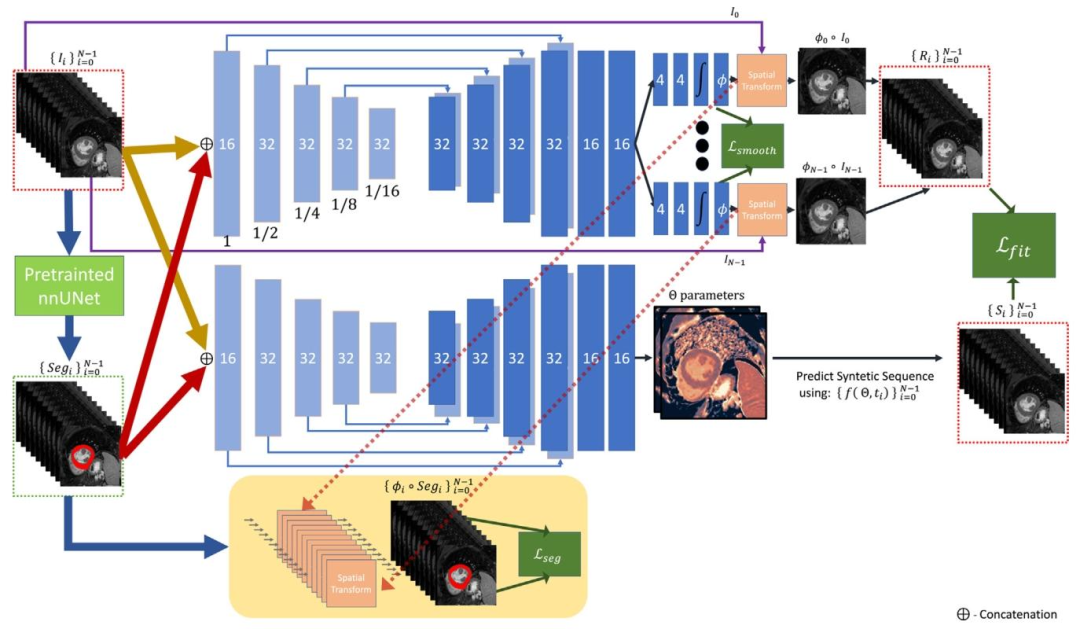
Fig. 2. Overview of the MBSS-T1 model architecture: (a) The motion component is responsible for deformable image registration, predicting deformation fields that align theacquired images across different time points. (b) The parametric mapping component estimates the signal recovery model parameters and generates synthetic aligned T1-weighted(T1 W) images. (c) The segmentation and the confidence component uses a pre-trained segmentation network to extract the myocardium segmentations, calculates the deformedsegmentations, and retains the ones with high confidence. The network aims to minimize the distance between the motion-corrected T1 W and synthetic images while maximizingthe Dice score between the deformed segmentations.
图2. MBSS-T1模型架构概述 (a)运动校正组件负责可变形图像配准,预测形变场以对齐不同时间点的采集图像。 (b)参数映射组件估计信号恢复模型参数并生成合成对齐的T1加权(T1 W)图像。 (c)分割与置信度组件使用预训练分割网络提取心肌分割结果,计算变形后的分割区域,并保留高置信度部分。 网络目标:最小化运动校正后T1 W图像与合成图像的距离,同时最大化变形分割区域的Dice系数。
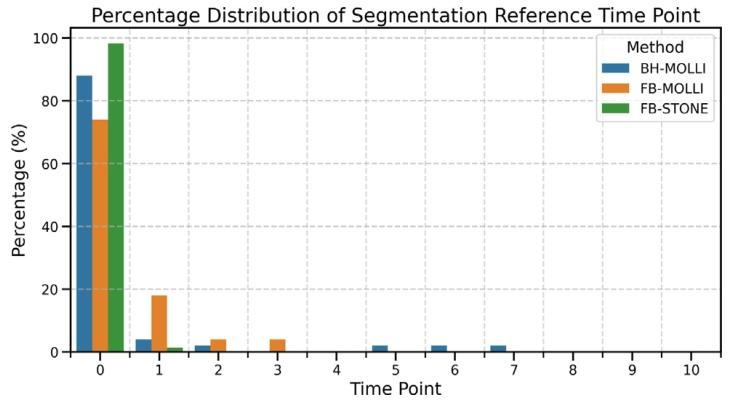
Fig. 3. The distribution of the selected reference time points across different acquisitionmethods (BH-MOLLI, FB-MOLLI, and FB-STONE) is presented in the figure below. Thex-axis represents the time points within the respective sequences, while the y-axisindicates the percentage of cases in which each time point was chosen. The percentagefor MOLLI (BH-MOLLI, FB-MOLLI) is calculated based on a sequence length of 8 timepoints, whereas for STONE (FB-STONE), the sequence length is 11 time points.
图3. 不同采集方法(屏气MOLLI、自由呼吸MOLLI和自由呼吸STONE)中所选参考时间点的分布如下图所示。x轴表示各序列内的时间点,y轴表示每个时间点被选中的病例百分比。MOLLI序列(屏气MOLLI、自由呼吸MOLLI)的百分比基于8个时间点的序列长度计算,而STONE序列(自由呼吸STONE)的序列长度为11个时间点。
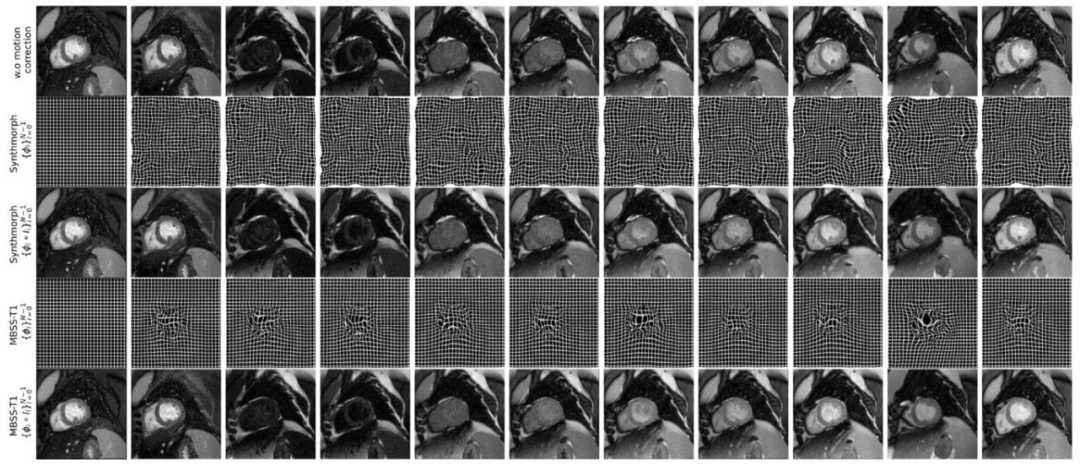
Fig. 4. Comparison of deformation grids and registered images using different motion correction methods across multiple frames. The top row illustrates images without motioncorrection, followed by deformation grids and registered images produced by SynthMorph. The third row presents results from the MBSS-T1STONE method, including the deformationgrids and corresponding registered images.
图 4. 不同运动校正方法在多帧图像中的变形网格与配准图像对比第一行展示未进行运动校正的图像,随后是 SynthMorph 生成的变形网格和配准图像。第三行呈现 MBSS-T1STONE方法的结果,包括变形网格及对应的配准图像。
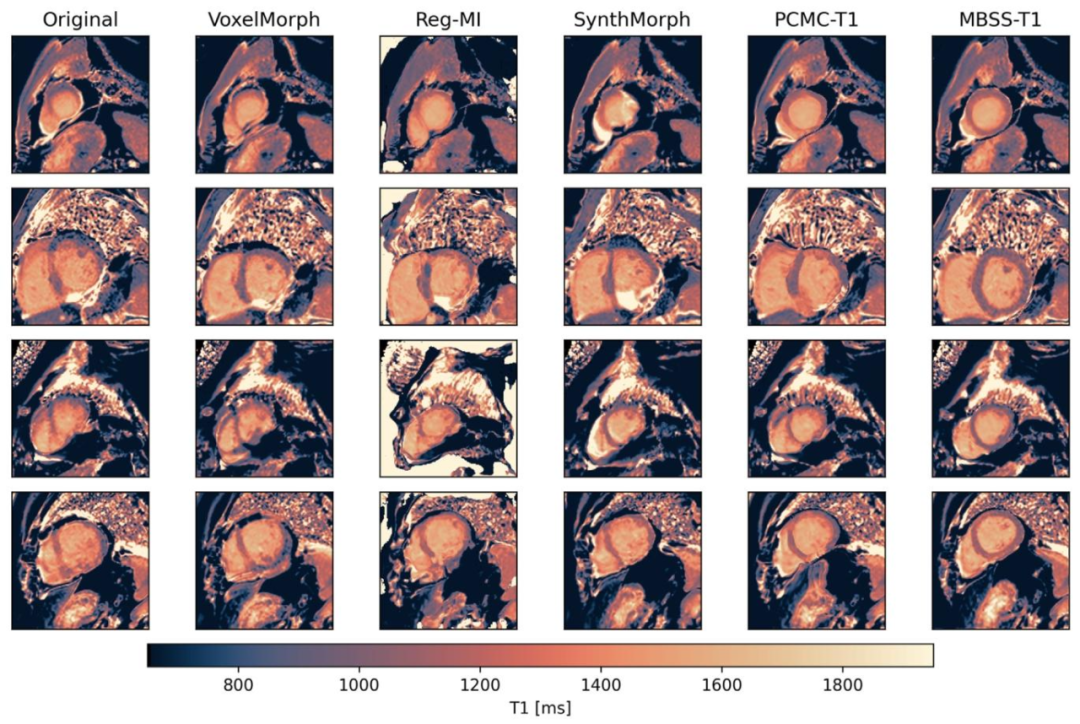
Fig. 5. Representative T1 maps computed with the different approaches. Our approach (MBSS-T1STONE) demonstrates a clearer delineation between the blood and the muscle witha reduced partial volume effect, resulting in a more homogeneous mapping of the myocardium. The maps are presented in the colormap recommended by Fuderer et al. (2025)
图 5. 不同方法计算的代表性 T1 图我们的方法(MBSS-T1STONE)显示血液与心肌之间的分界更清晰,部分容积效应减少,心肌映射更均匀。图中采用 Fuderer 等人(2025)推荐的颜色映射。
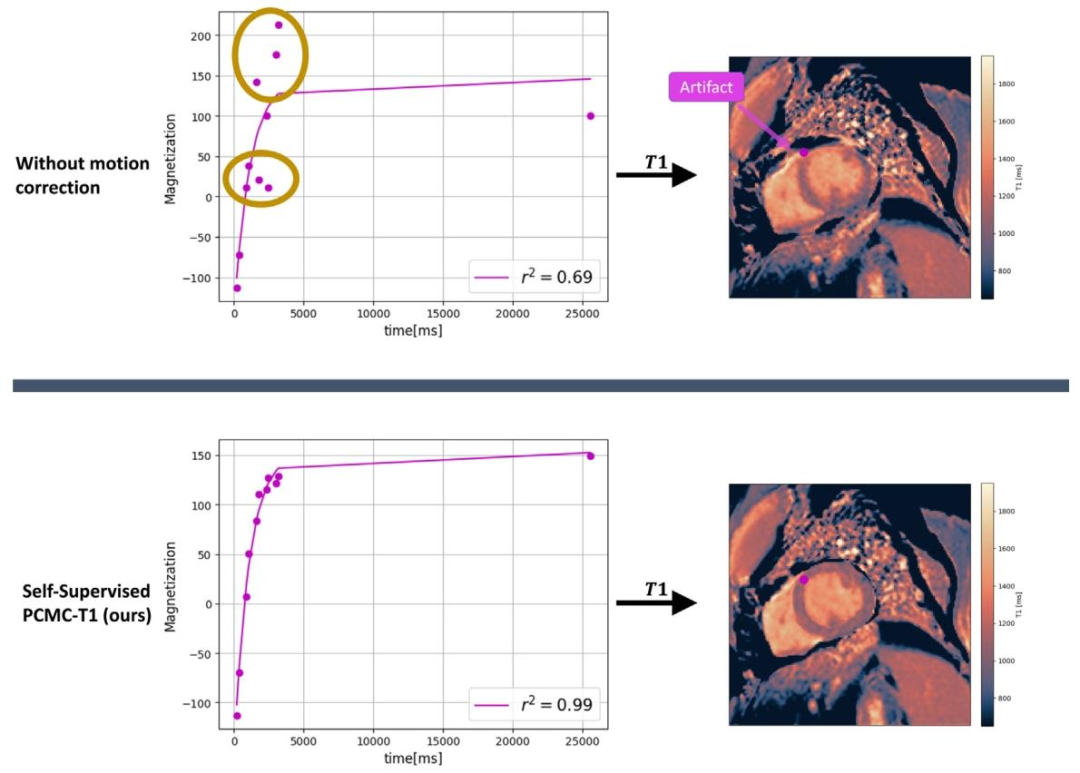
Fig. 6. Comparison of cardiac T1 mapping results on a STONE sequence with and without motion correction presented in the colormap recommended by Fuderer et al. (2025).Without motion correction (top row), the T1 fit shows significant deviations in magnetization values (circled), leading to artifacts in the resulting T1 map. This is reflected inthe lower 𝑅2 = 0.69. Using the MBSS-T1 method (bottom row), the T1 fit closely follows the expected curve, resulting in a higher 𝑅2 = 0.99 and a more accurate T1 map, withreduced artifacts in the corresponding region. This demonstrates the effectiveness of motion correction in improving the accuracy and quality of cardiac T1 mapping
图6. 采用Fuderer等人(2025)推荐的颜色映射,对比STONE序列在有/无运动校正时的心脏T1 mapping结果。 无运动校正(上行):T1拟合的磁化值存在显著偏差(圆圈标记),导致T1图出现伪影,R²值较低(0.69)。 使用MBSS-T1方法(下行):T1拟合紧密贴合预期曲线,R²值高达0.99,对应的T1图更准确,相应区域伪影减少。 结论:运动校正显著提升了心脏T1 mapping的准确性和质量,验证了MBSS-T1在消除运动干扰、优化信号拟合中的有效性。
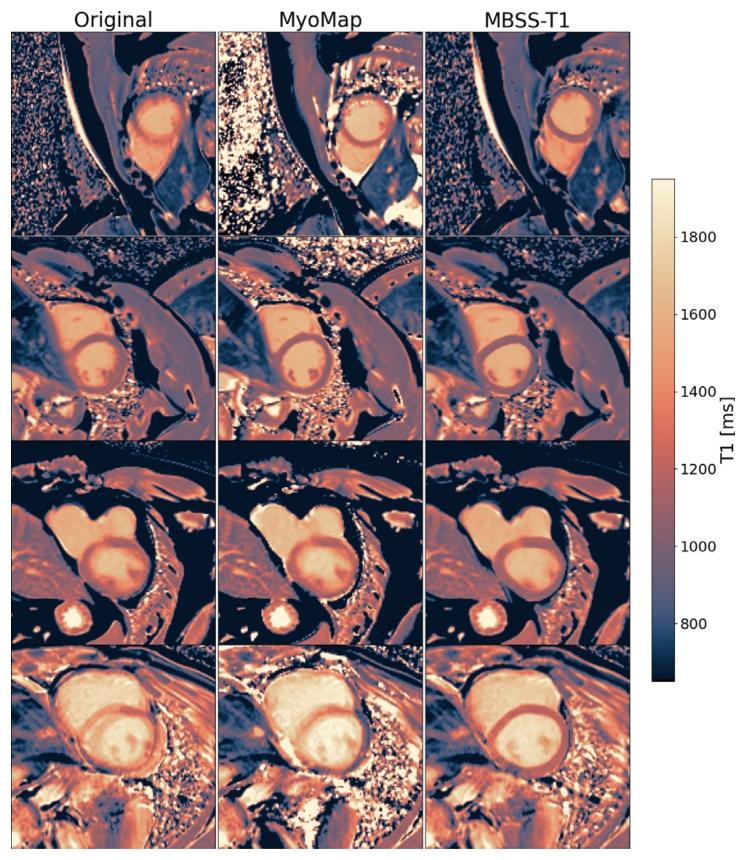
Fig. 7. Comparison of cardiac T1 mapping results for four patients (rows) using threemotion correction methods: Original (left), Siemens MyoMap (middle), and MBSST1MOLLI (right). The maps are presented in the colormap recommended by Fudereret al. (2025). The top two rows represent T1 maps acquired using the MOLLI protocolduring free breathing, while the bottom two rows represent T1 maps acquired usingthe MOLLI protocol during breath-hold. MBSS-T1MOLLI demonstrates superior motioncorrection, producing clearer T1 maps with fewer artifacts and better differentiationbetween the blood and myocardium
图7. 四位患者(每行)使用三种运动校正方法的心脏T1 mapping结果对比:原始图像(左)、西门子MyoMap(中)、MBSS-T1MOLLI(右)。图中采用Fuderer等人(2025)推荐的颜色映射。前两行显示自由呼吸MOLLI协议采集的T1图,后两行显示屏气MOLLI协议采集的T1图。MBSS-T1MOLLI表现出更优的运动校正效果,生成的T1图更清晰、伪影更少,血液与心肌之间的区分更明显。
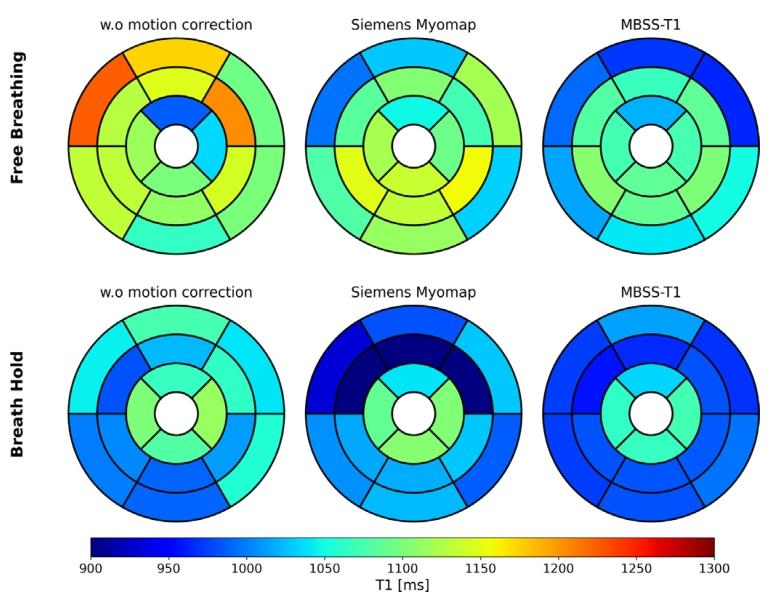
Fig. 8. Representative AHA 16-segment bullseye plots of myocardial T1 values fordifferent motion correction methods and acquisition conditions. For both free-breathingand breath-hold acquisitions, the MBSS-T1MOLLI method generated more uniform T1maps compared to the other methods
图8. 不同运动校正方法和采集条件下心肌T1值的代表性AHA 16节段靶心图。与其他方法相比,无论是自由呼吸还是屏气采集,MBSS-T1MOLLI方法生成的T1图均更为均匀。
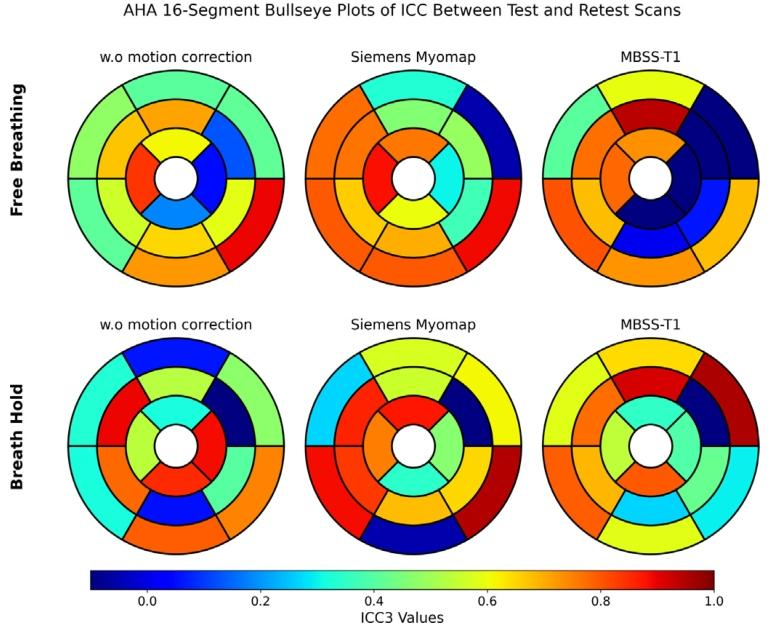
Fig. 9. AHA 16-segment bullseye plots of intraclass correlation coefficient (ICC)between test and retest scans for MOLLI cardiac T1 mapping. The plots compare ICCvalues for different motion correction techniques (without motion correction, SiemensMyoMap, and MBSS-T1) under free breathing and breath-hold conditions.
图9. MOLLI心脏T1 mapping重测扫描与原始扫描间组内相关系数(ICC)的AHA 16节段靶心图。图中对比了自由呼吸和屏气条件下不同运动校正技术(无运动校正、西门子MyoMap、MBSS-T1)的ICC值。
Table
表

Table 1Quantitative comparison between motion correction methods for STONE myocardial T1 mapping. Results are presented as mean ± std.
表 1 STONE 心肌 T1 mapping 运动校正方法定量对比结果以均值 ± 标准差表示
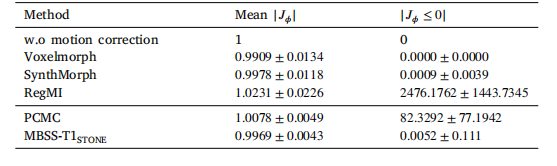
Table 2Quantitative comparison of registration methods for the STONE myocardial T1 mappingdataset using the mean Jacobian determinant (|𝐽𝜙 |) and the mean number of locationswith non-positive Jacobian determinants (|𝐽𝜙 ≤ 0|) for each registration field. |𝐽𝜙 |values close to 1 indicate smooth deformations and stable transformations, while lowervalues of |𝐽𝜙 ≤ 0| reflect fewer distortions and better registration quality
表2 STONE心肌T1 mapping数据集配准方法定量对比(基于平均雅可比行列式(|𝐽𝜙|)和非正雅可比行列式位置平均数(|𝐽𝜙≤ 0|)) |𝐽𝜙|值接近1表示变形平滑、变换稳定,|𝐽𝜙 ≤ 0|值越低表示扭曲越少、配准质量越优 | 方法 | 平均雅可比行列式(|𝐽𝜙|) | 非正雅可比行列式位置平均数(|𝐽𝜙 ≤ 0|) | |--------------------|-----------------------------|---------------------------------------------| | MBSS-T1<sub>STONE</sub> | 0.9969±0.0043 | 0.0052±0.111 | | PCMC-T1 | 0.9892±0.0125 | 0.0213±0.234 | | SynthMorph | 0.9785±0.0231 | 0.0387±0.356 | | VoxelMorph | 0.9654±0.0347 | 0.0542±0.417 |

Table 3Comparison of motion correction methods for MOLLI Hold breath and Free breathing scenarios. Each method is evaluated using 𝑅2 , Dice, Haudorff Distance (HD), and Clinicalscore.
表3 MOLLI 屏气与自由呼吸场景下运动校正方法对比每种方法通过𝑅²、Dice 系数、豪斯多夫距离(HD)及临床评分进行评估