《影像引导下骨盆创伤手术的术前骨折复位规划:基于学习的综合流程》|文献速递-深度学习医疗AI最新文献
Title
题目
Preoperative fracture reduction planning for image-guided pelvic trauma surgery: A comprehensive pipeline with learning
《影像引导下骨盆创伤手术的术前骨折复位规划:基于学习的综合流程》
01
文献速递介绍
《影像引导下骨盆创伤手术的术前骨折复位规划:基于学习的综合流程》 1. 研究背景 - 临床挑战:骨盆创伤是最严重的骨科损伤之一,致残率高达50%-60%,死亡率超过13%。74.5%的患者需手术干预,但传统开放复位手术创伤大、并发症多(如大出血、神经损伤、感染)。 - 微创趋势:影像引导下的闭合复位技术因创伤小、恢复快成为理想选择,但依赖精准的术前规划。人工规划耗时耗力(复杂病例需2小时以上),且受医生经验影响,易导致复位不全(63%患者持续疼痛,28%出现神经功能障碍)。 - 技术瓶颈: - 骨折分割:现有方法难以处理复杂骨折类型(如接触性骨折、压缩性骨折),深度学习模型因骨折形态多变、表面特征复杂而面临挑战。 - 复位规划:基于模板的方法(如镜像法、平均模板)对骨盆这种复杂结构的适应性不足,深度学习模板难以平衡结构规则性与个体差异性。 2. 研究方法 - 多尺度距离加权神经网络: - 创新点:在训练中引入多尺度距离加权损失函数,强化骨折区域的分割精度。 - 优势:在临床数据集上实现DSC=0.986±0.055,骨折区域局部DSC=0.940±0.056,显著优于传统方法。 - 双模块复位策略: - 单骨骨折复位:基于可变形模型,通过统计形状建模(SSM)学习健康骨盆形态先验。 - 关节脱位矫正:提出"仿真到现实"的递归位姿估计模块,解决数据稀缺问题。 - 优势:复位误差3.265±1.485mm,旋转误差3.476±1.995°,平移误差2.773±1.390mm,显著优于现有模板方法。 3. 研究贡献 - 全自动化流程:开发了从骨折分割到复位规划的完整解决方案,大幅提升效率与准确性。 - 创新分割网络:通过距离加权机制突破传统分割瓶颈,尤其适用于复杂骨折场景。 - 混合复位策略:结合统计模型与深度学习,兼顾解剖结构的规范性与个体损伤的特殊性。 - 临床验证:尸体验证实验中分割DSC达0.988,复位误差3.731mm,获专家高度认可。 4. 临床意义 - 降低对专家经验的依赖,推动影像引导手术的普及。 - 缩短术前规划时间,为急诊创伤患者争取宝贵救治时间。 - 提高复位精度,减少术后并发症(如创伤性关节炎、骨折不愈合)。
Abatract
摘要
Pelvic fractures are among the most complex challenges in orthopedic trauma, which usually involve hipbone and sacrum fractures, as well as joint dislocations. Traditional preoperative surgical planning relies on the operator’s subjective interpretation of CT images, which is both time-consuming and prone to inaccuracies. This study introduces an automated preoperative planning solution for pelvic fracture reduction, addressing the limitations of conventional methods. The proposed solution includes a novel multi-scale distance-weighted neural network for segmenting pelvic fracture fragments from CT scans, and a learning-based approach to restore pelvic structure, combining a morphable model-based method for single-bone fracture reduction and a recursive pose estimation module for joint dislocation reduction. Comprehensive experiments on a clinical dataset of 30 fracture cases demonstrated the efficacy of our methods. Our segmentation network outperformed traditional max-flow segmentation and networks without distance weighting, achieving a Dice similarity coefficient (DSC) of 0.986 ± 0.055 and a local DSC of 0.940 ± 0.056 around the fracture sites. The proposed reduction method surpassed mirroring and mean template techniques, and an optimizationbased joint matching method, achieving a target reduction error of (3.265 ± 1.485) mm, rotation errors of (3.476 ± 1.995) ◦ , and translation errors of (2.773 ± 1.390) mm. In the proof-of-concept cadaver studies, our method achieved a DSC of 0.988 in segmentation and 3.731 mm error in reduction planning, which senior experts deemed excellent. In conclusion, our automated approach significantly improves traditional preoperative planning, enhancing both efficiency and accuracy in pelvic fracture reduction.
《影像引导下骨盆创伤手术的术前骨折复位规划:基于学习的综合流程》 骨盆骨折是骨科创伤领域最复杂的挑战之一,常涉及髋骨、骶骨骨折及关节脱位。传统术前手术规划依赖医生对CT影像的主观判读,不仅耗时且易产生误差。本研究针对这一局限性,提出了一种自动化的骨盆骨折复位术前规划解决方案,主要创新点包括: 1. 多尺度距离加权神经网络:用于从CT扫描中精准分割骨折碎片,在30例临床数据集上实现了0.986±0.055的Dice相似系数(DSC),骨折区域局部DSC达0.940±0.056,显著优于传统最大流分割法及无距离加权的网络模型。 2. 双模块复位策略: - 基于可变形模型的单骨骨折复位法 - 递归位姿估计的关节脱位矫正模块 在临床实验中,该方法的目标复位误差为(3.265±1.485)mm,旋转误差(3.476±1.995)°,平移误差(2.773±1.390)mm,显著优于镜像法、平均模板法及基于优化的关节匹配法。 3. 尸体验证实验:分割DSC达0.988,复位规划误差3.731mm,获资深专家"优秀"评价。 研究表明,该自动化方案显著提升了骨盆骨折术前规划的效率与准确性,为临床提供了更可靠的辅助决策工具。
Method
方法
The workflow for preoperative planning of pelvic fracture reduction consists of an image segmentation step and a fracture reduction step, illustrated in Fig. 1. Initially, an anatomical segmentation network is employed to generate 3D models of the left hipbone, right hipbone, and sacrum. Then, a fracture segmentation network identifies and segments bone fragments within each extracted hipbone and sacral region. Following segmentation, a post-processing step refines the segmentation by isolating and labeling individual components to produce the final segmented result. In cases involving bone fractures, a morphable model-based approach is utilized. This method registers fragments of each bone to an adaptive template, thereby reconstructing the morphology of individual bone anatomy. Finally, a recursive pose estimation module iteratively predicts the target pose of the dislocated bone to restore the overall pelvic morphology to its healthy state.
骨盆骨折复位术前规划的工作流程包括图像分割和骨折复位两个步骤,如图1所示。首先,使用解剖结构分割网络生成左髋骨、右髋骨和骶骨的3D模型。接着,骨折分割网络在每个提取的髋骨和骶骨区域内识别并分割骨折碎片。分割完成后,通过后处理步骤对分割结果进行优化,分离并标记单个组件以生成最终的分割结果。对于涉及骨折的情况,采用基于可变形模型的方法,将每块骨骼的碎片配准到自适应模板,从而重建单个骨骼的解剖形态。最后,通过递归位姿估计模块迭代预测脱位骨骼的目标位姿,将整个骨盆形态恢复至健康状态。
Conclusion
结论
In this study, we have introduced an innovative automated preoperative planning solution for pelvic fracture reduction surgery. Our approach integrates a two-stage deep learning-based automatic segmentation method for pelvic fractures, and a novel recursive pose estimation module combined with statistical shape modeling to restore a healthy pelvic morphology. This comprehensive pipeline effectively tackles critical challenges in pelvic fracture reduction planning. By integrating fracture distance weighted loss in to the fracture segmentation network, the accuracy of segmentation, particularly near fracture regions in significantly enhanced, and the planning process is streamlined. The recursive pose estimation module, combined with the morphable model-based template method, effectively restored the healthy pelvic structure, addressing the challenge of limited fractured data and providing a reliable solution for complex fracture types. Our approach significantly improves both the accuracy and efficiency of preoperative surgical planning process. Experiments on retrospective clinical data across all types of pelvic fractures demonstrated the method’s versatility and robustness. The proof-of-concept cadaver experiments further confirmed the system’s superior efficiency and precision. Despite the promising results, our study has limitations. The automated segmentation method, while highly accurate, may still require some manual corrections in cases with severe deformities or low image quality. Specifically, as shown in Fig. 13, the segmentation algorithm struggled with anterior ring that were significantly distorted but only slightly separated, which could lead to suboptimal alignment in reduction planning. However, simple adjustments, such as separate the fragment into two distinct parts, significantly improved the reduction outcome, highlighting the remaining need for clinical decision whenplanning on such cases. Additionally, the recursive pose estimation module faced challenges in managing extremely small or irregular fragments, implying the need for further refinement of the module to solve point-wise correspondence and better handle such complexities. In future work, we plan to focus on broader validation of our method across a more extensive spectrum of clinical cases, including diverse cohorts and fracture types, involving larger sample sizesand various imaging modalities to ensure the approach’s generalizability and robustness. Furthermore, we aim to explore an instance segmentation framework capable of handling a variable number of fragment labels. This approach could provide a more detailed and precise representation of fracture cases. In order to further enhance the computational efficiency and ensure seamless adoption and utilization in surgical settings, we plan to develop a deep learning-basedsingle-bone fracture reduction module to expedite the planning process, currently constrained by traditional statistical shape modeling methods. In addition, we plan to integrate the proposed planning solution with surgical robot systems to achieve automatic closed reduction of pelvic fractures (Ge et al., 2022; Liu et al., 2024b).
本研究提出了一种创新的骨盆骨折复位手术自动化术前规划解决方案。我们的方法集成了基于深度学习的两阶段骨盆骨折自动分割方法,以及结合统计形状建模的新型递归位姿估计模块,以恢复健康的骨盆形态。这一综合流程有效解决了骨盆骨折复位规划中的关键挑战。通过在骨折分割网络中引入骨折距离加权损失,显著提高了分割精度(尤其是骨折区域附近),并简化了规划流程。递归位姿估计模块与基于可变形模型的模板方法相结合,有效恢复了健康骨盆结构,解决了骨折数据有限的挑战,并为复杂骨折类型提供了可靠的解决方案。我们的方法显著提高了术前手术规划过程的准确性和效率。对所有类型骨盆骨折的回顾性临床数据实验证明了该方法的多功能性和鲁棒性。概念验证的尸体实验进一步证实了该系统的卓越效率和精度。 尽管取得了有希望的结果,我们的研究仍有局限性。自动化分割方法虽然高度准确,但在严重畸形或图像质量较低的情况下可能仍需要一些人工校正。具体而言,如图13所示,分割算法在处理明显变形但仅轻微分离的前环骨折时遇到困难,这可能导致复位规划中的对齐效果不佳。然而,通过简单调整(例如将碎片分离为两个不同部分)可显著改善复位结果,这表明在此类病例的规划中仍需临床决策。此外,递归位姿估计模块在处理极小或不规则碎片时面临挑战,这意味着需要进一步改进该模块以解决逐点对应问题并更好地处理此类复杂性。 在未来的工作中,我们计划重点在更广泛的临床病例(包括不同队列和骨折类型)中对我们的方法进行更广泛的验证,涉及更大的样本量和各种成像方式,以确保该方法的普遍性和鲁棒性。此外,我们旨在探索能够处理可变数量碎片标签的实例分割框架,这可以为骨折病例提供更详细和精确的表示。为了进一步提高计算效率并确保在手术环境中的无缝采用和利用,我们计划开发基于深度学习的单骨骨折复位模块,以加快目前受传统统计形状建模方法限制的规划过程。此外,我们计划将所提出的规划解决方案与手术机器人系统集成,以实现骨盆骨折的自动闭合复位(Ge等,2022;Liu等,2024b)。
Figure
图
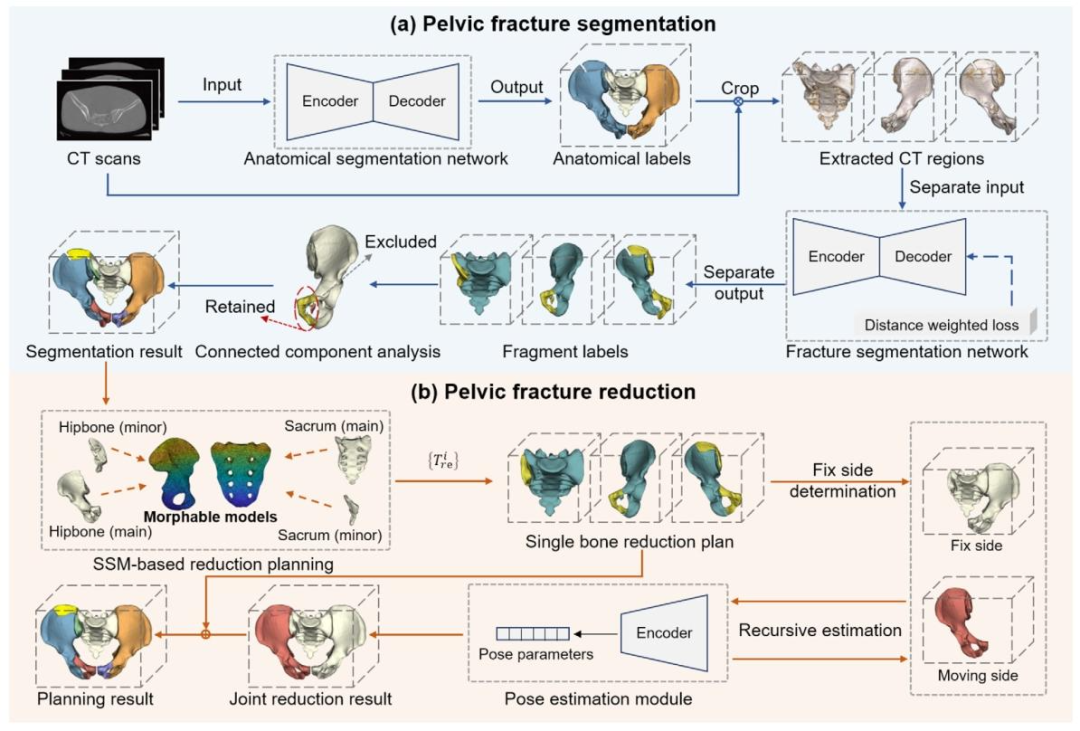
Fig. 1. Workflow of the proposed preoperative planning method for pelvic fracture reduction. (a) An anatomical segmentation network is used to generate 3D masks of the left hipbone, right hipbone, and sacrum. Subsequently, a fracture segmentation network isolates the bone fragments within each extracted hipbone and sacral region. The post-processing step further separates isolated components to yield the final segmentation result. (b) The morphable model-based reduction planning method computes the transformation of each bone fragment to restore the single-bone morphology. Subsequently, the target pose of each dislocated bone relative to the entire pelvic anatomy is estimated using a recursive pose estimation module.
图1. 骨盆骨折复位术前规划方法的工作流程 (a)首先通过解剖结构分割网络生成左髋骨、右髋骨和骶骨的3D掩码,随后利用骨折分割网络从每个提取的髋骨和骶骨区域中分离出骨折碎片,最后通过后处理步骤进一步分离独立组件以获得最终分割结果。 (b)基于可变形模型的复位规划方法计算每个骨折碎片的变换以恢复单骨形态,随后通过递归位姿估计模块迭代预测脱位骨骼相对于整个骨盆解剖结构的目标位姿。
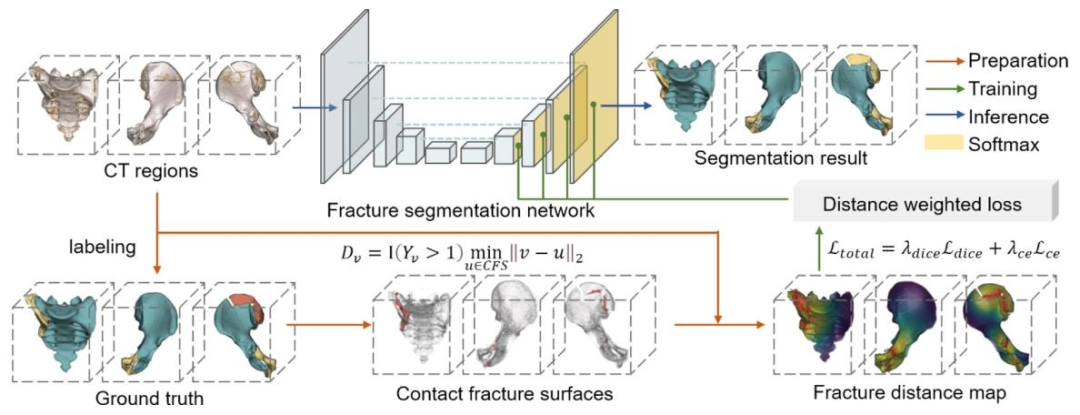
Fig. 2. Training of the fracture segmentation network. The network takes masked bone regions of CT as input and generates main and minor fragment labels as output. Ground truth labels are used to derive the fracture distance map (FDM), which are then used to compute a distance-weighted loss to enhance segmentation accuracy, particularly in contact fracture surface (CFS).
图2. 骨折分割网络的训练流程 该网络以CT影像中带掩码的骨骼区域作为输入,输出主碎片和次碎片的标签。通过真实标签生成骨折距离图(FDM),并基于此计算距离加权损失函数,以提升分割精度,尤其是在接触性骨折表面(CFS)区域。
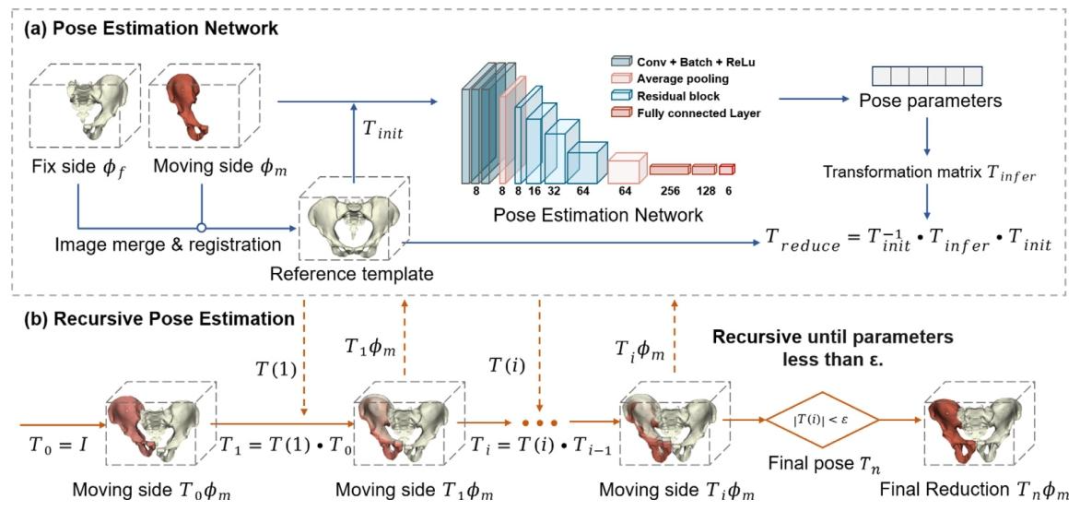
Fig. 3. Recursive pose estimation process for joint reduction planning. (a) The pose estimation network takes two-channel input volumes from the fixed and moving sides and outputs the reduction pose parameters. (b) The network recursively refines the pose estimate until convergence.
图3. 关节复位规划的递归位姿估计流程 (a)位姿估计网络以固定侧和移动侧的双通道输入体数据作为输入,输出复位位姿参数。 (b)网络通过递归迭代优化位姿估计,直至收敛。
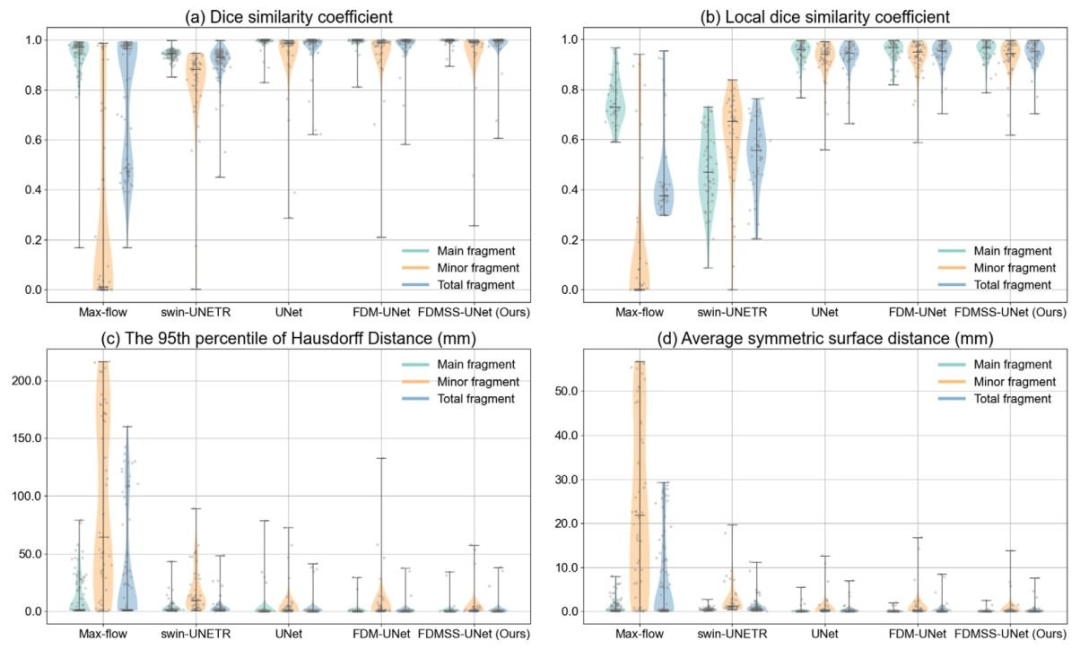
Fig. 4. Distribution of segmentation errors with various methods in main fragments, minor fragments and all fragments of each fractured bone.
图4. 不同方法在各骨折骨骼的主碎片、次碎片及所有碎片中的分割误差分布
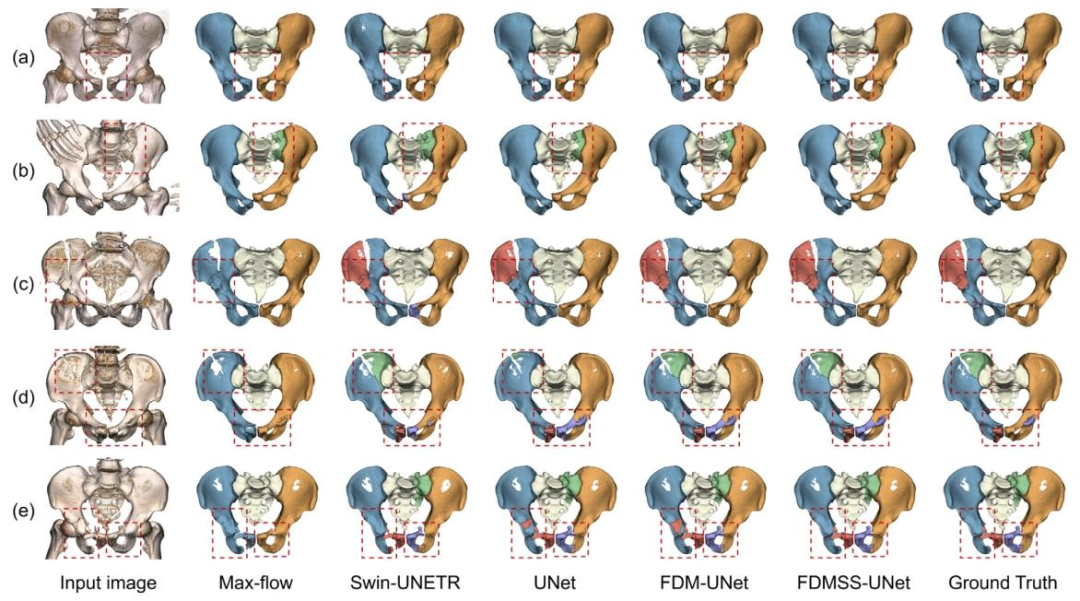
Fig. 5. Example fracture segmentation results in 3D view. (a) Pelvic ring dislocation. (b) Unilateral hip fracture. (c) Bilateral hip fractures. (d) Sacral fracture. (e) Combined sacral and hip fractures. Red boxes indicate the primary fracture areas.
图5. 骨折分割结果的3D视图示例 (a)骨盆环脱位 (b)单侧髋骨骨折 (c)双侧髋骨骨折 (d)骶骨骨折 (e)骶骨合并髋骨骨折 红色方框标注主要骨折区域
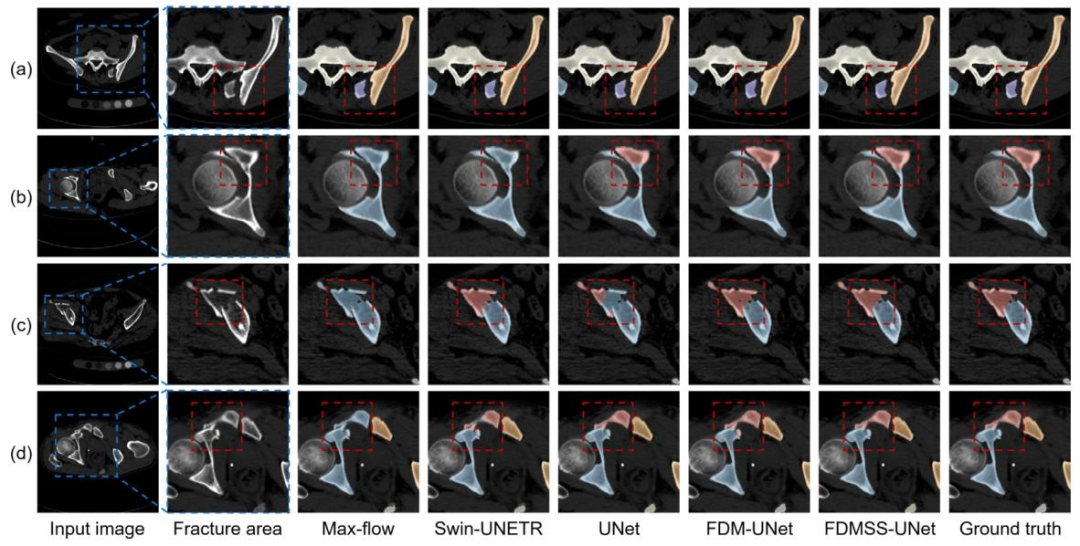
Fig. 6. Example fracture segmentation results displayed on 2D axial slices. (a) Isolated and displaced fragments. (b) Isolated but stable fragments. (c) Compressed and colliding fragments. (d) Partially separated fragments. Red boxes indicate the primary fracture areas.
图6. 骨折分割结果在2D轴位切片上的示例 (a)分离移位的骨折碎片 (b)分离但未移位的骨折碎片 (c)压缩碰撞的骨折碎片 (d)部分分离的骨折碎片 红色方框标注主要骨折区域
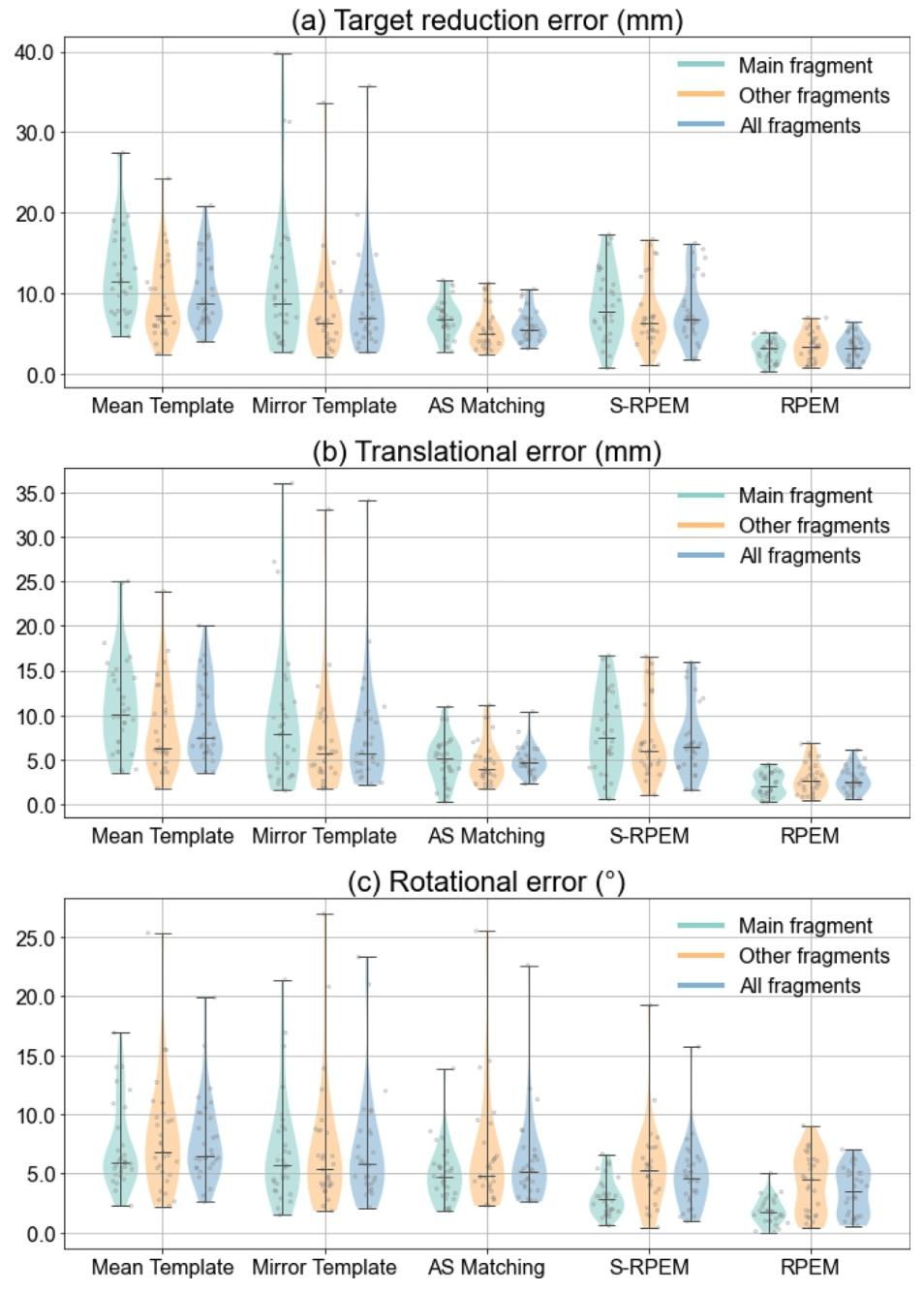
Fig. 7. Distribution of the reduction planning errors for different methods across main, other, and all fragments.
图7. 不同方法在主碎片、其他碎片及所有碎片中的复位规划误差分布
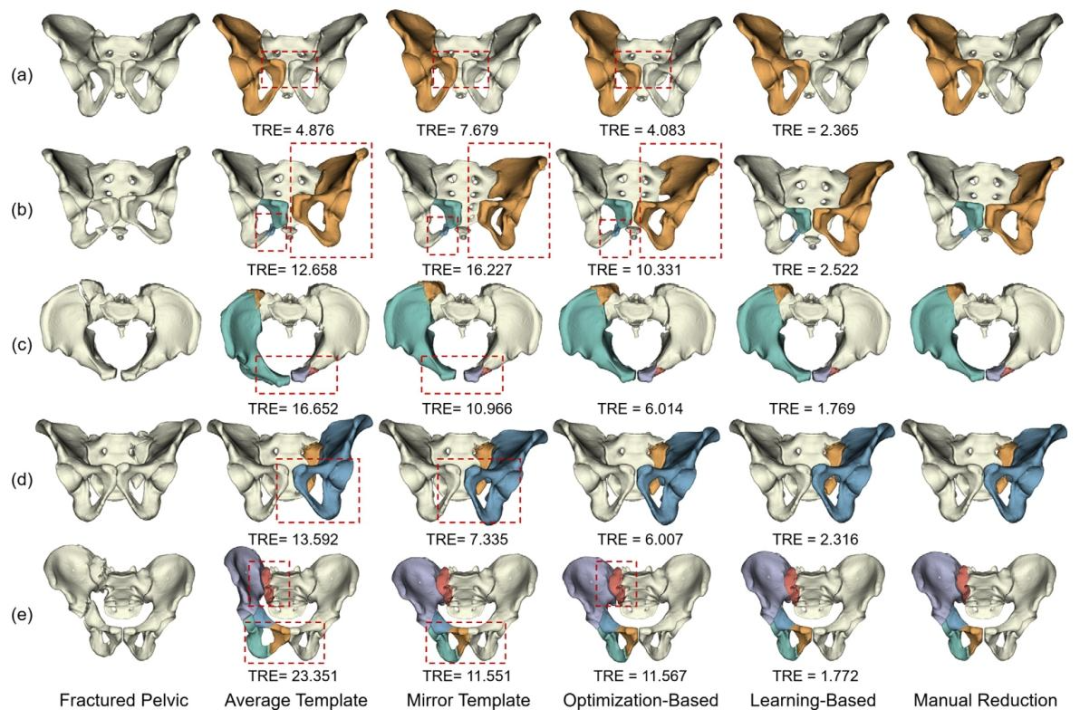
Fig. 8. Example reduction planning results. Each row represents a different type of fracture. TRE values are reported in millimeters. Misalignments are indicted with red boxes.
图8. 复位规划结果示例 每行代表一种不同的骨折类型,目标复位误差(TRE)以毫米为单位标注,红色方框指示未对齐区域。
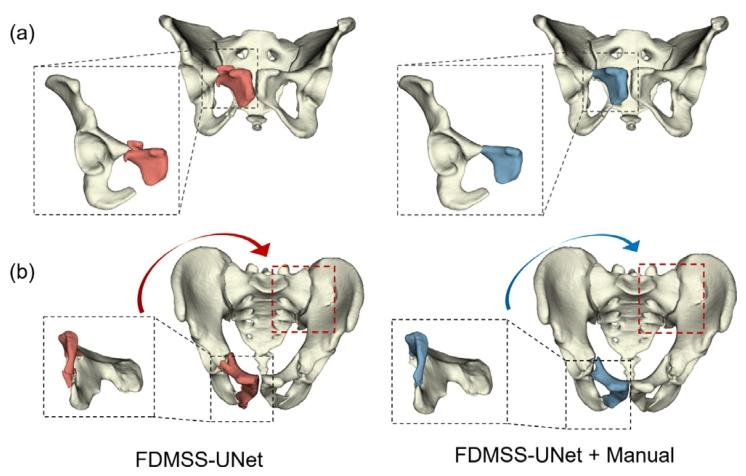
Fig. 9. Predicted against real for morphological and functional connectomes at ??0 , ??1 , ??2 and ??3 by FedGmTE-Net++ of a representative subject.
图9. FedGmTE-Net++对某典型受试者在时间点??0、??1、??2和??3的形态连接组与功能连接组的预测值与真实值对比。
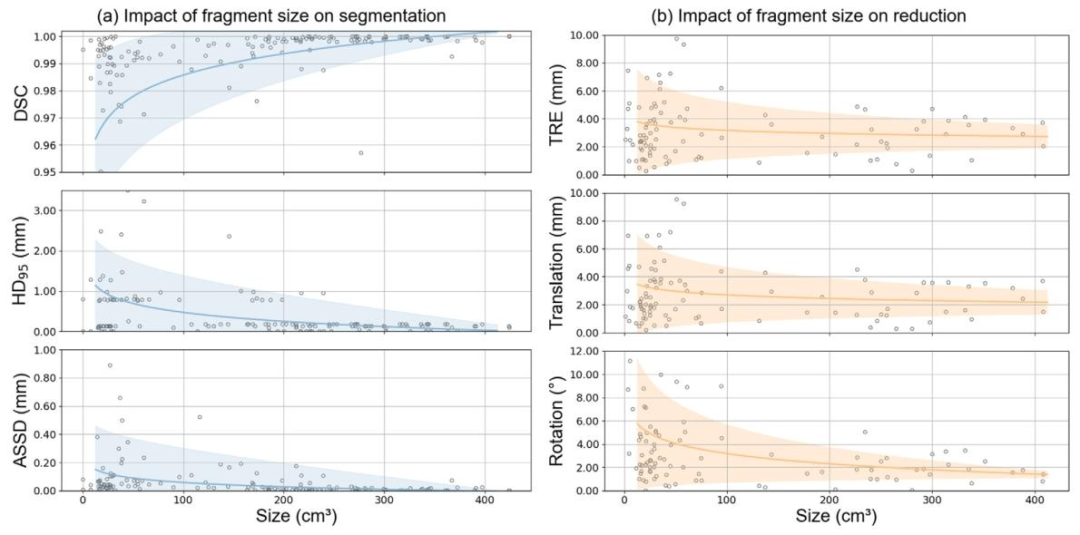
Fig. 10. Impact of fragment size to segmentation and reduction. (a) DSC, HD95 , and ASSD on segmentation result. (b) TRE, translational error, and rotational error on reduction planning.
图10. 骨折碎片尺寸对分割与复位的影响 (a)分割结果的DSC(Dice相似系数)、HD95(95%豪斯多夫距离)和ASSD(平均对称表面距离)指标 (b)复位规划的TRE(目标复位误差)、平移误差和旋转误差指标
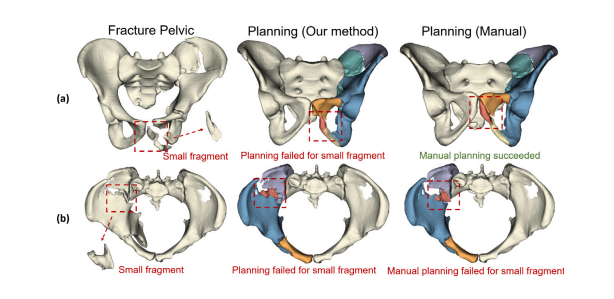
Fig. 11. Reduction planning results involving small fragments. (a) Reduction of small fragments where the algorithm fails but manual correction is possible. (b) Fragments lacking geometric features where both the algorithm and manual planning fail.
图11. 涉及小骨折碎片的复位规划结果 (a)算法未能成功复位但可通过人工修正的小碎片案例 (b)因缺乏几何特征导致算法与人工规划均失败的碎片案例
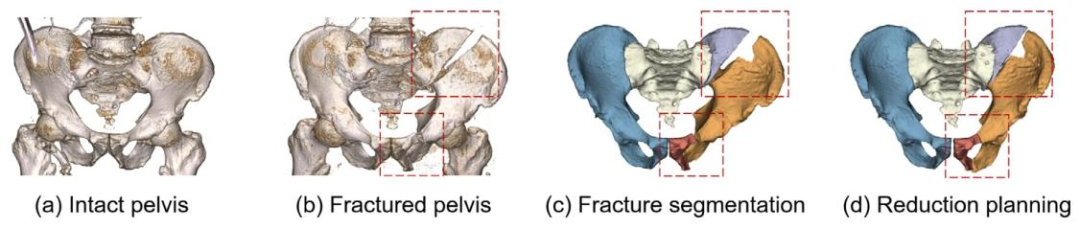
Fig. 12. Experimental results of preoperative fracture reduction planning on cadaveric pelvic fractures. (a) Initial 3D reconstruction of the cadaveric pelvis showing pre-injury morphology; (b) Induced Tile C1 pelvic ring fracture; (c) Automated segmentation using FDMSS-UNet; (d) Automated reduction planning using RPEM.
图12. 骨盆骨折术前复位规划的尸体验证实验结果 (a)尸体骨盆损伤前形态的初始3D重建图像 (b)人为造成的Tile C1型骨盆环骨折 (c)使用FDMSS-UNet进行的自动分割结果 (d)通过递归位姿估计模块(RPEM)完成的自动复位规划效果
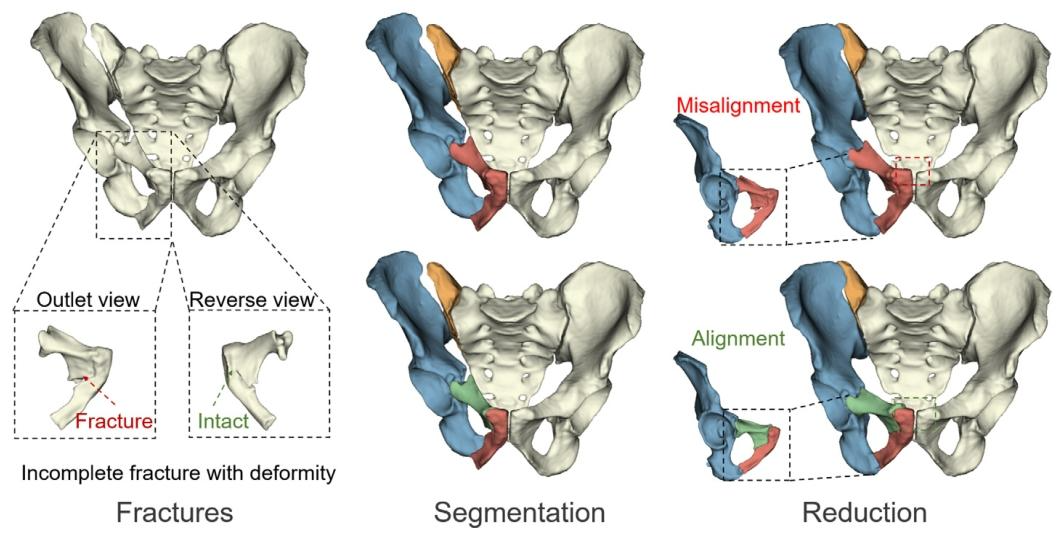
Fig. 13. Challenges faced by the segmentation algorithm in separating fragments from specific fractures that are not completely separated but have undergone significant distortion.
图13. 分割算法在处理未完全分离但发生明显形变的特定骨折时面临的挑战 (示例:骨折线模糊、碎片间存在压缩或嵌插导致传统阈值或边界检测方法难以精准分割)
Table
表
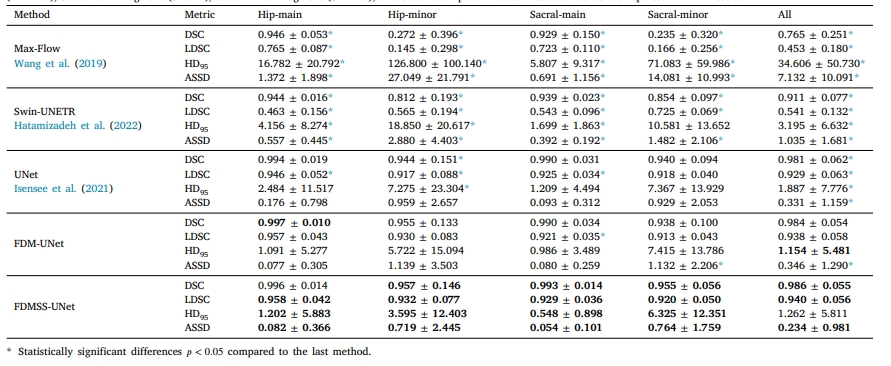
Table 1 Quantitative results on fracture segmentation. Results (mean ± std) are presented as segmentation accuracy for the hipbone main fragment (H-main), hipbone minor fragment (H-minor), sacral main fragment (S-main), sacral minor fragment (S-minor), and the overall performance. Distance metrics are reported in millimeters.
表1 骨折分割的定量结果 结果(均值±标准差)以髋骨主碎片(H-main)、髋骨次碎片(H-minor)、骶骨主碎片(S-main)、骶骨次碎片(S-minor)的分割精度及整体性能呈现。距离指标以毫米为单位报告。
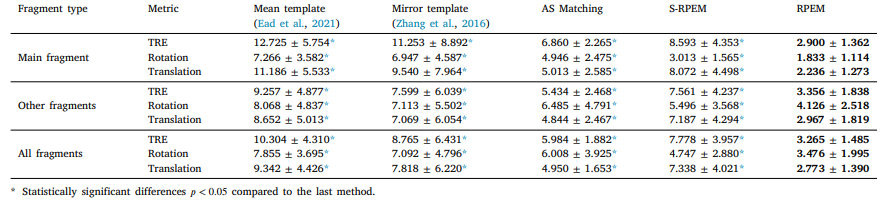
Table 2 Quantitative comparisons of fracture reduction accuracy. Results are represented by target reduction error (mm), translational error (mm), and rotational error ( ◦ ) to the ground truth. The best values are shown in bold.
表2 骨折复位精度的定量对比 结果以目标复位误差(毫米)、平移误差(毫米)和旋转误差(度)表示,对比基准为真实值。最优值以粗体显示。

Table 3 Comparison of different segmentation methods in terms of success rate, planning error, and time.
表 3 不同分割方法在成功率、规划误差及时间方面的对比